Ladina Erhart, Beat A Kaufmann, Baris Gencer, Philipp K Haager, Hajo Müller, Richard Kobza, Leonhard Held, Simon F Stämpfli
{"title":"左心室非压实性肾功能不全及预后。","authors":"Ladina Erhart, Beat A Kaufmann, Baris Gencer, Philipp K Haager, Hajo Müller, Richard Kobza, Leonhard Held, Simon F Stämpfli","doi":"10.5603/CJ.a2022.0105","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>While renal function has been observed to inversely correlate with clinical outcome in other cardiomyopathies, its prognostic significance in patients with left ventricular non-compaction cardiomyopathy (LVNC) has not been investigated. The aim of this study was to determine the prognostic value of renal function in LVNC patients.</p><p><strong>Methods: </strong>Patients with isolated LVNC as diagnosed by echocardiography and/or magnetic resonance imaging in 4 Swiss centers were retrospectively analyzed for this study. Values for creatinine, urea, and estimated glomerular filtration rate (eGFR) as assessed by the CKD-EPI 2009 formula were collected and analyzed by a Cox regression model for the occurrence of a composite endpoint (death or heart transplantation).</p><p><strong>Results: </strong>During the median observation period of 7.4 years 23 patients reached the endpoint. The ageand gender-corrected hazard ratios (HR) for death or heart transplantation were: 1.9 (95% confidence interval [CI] 1.4-2.6) for each increase over baseline creatinine level of 30 μmol/L (p < 0.001), 1.6 (95% CI 1.2-2.2) for each increase over baseline urea level of 5 mmol/L (p = 0.004), and 3.6 (95% CI 1.9-6.9) for each decrease below baseline eGFR level of 30 mL/min (p ≤ 0.001). The HR (log2) for every doubling of creatinine was 7.7 (95% CI 3-19.8; p < 0.001), for every doubling of urea 2.5 (95% CI 1.5-4.3; p < 0.001), and for every bisection of eGFR 5.3 (95% CI 2.4-11.6; p < 0.001).</p><p><strong>Conclusions: </strong>This study provides evidence that in patients with LVNC impairment in renal function is associated with an increased risk of death and heart transplantation suggesting that kidney function assessment should be standard in risk assessment of LVNC patients.</p>","PeriodicalId":2,"journal":{"name":"ACS Applied Bio Materials","volume":" ","pages":"781-789"},"PeriodicalIF":4.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10635721/pdf/","citationCount":"0","resultStr":"{\"title\":\"Renal dysfunction and outcome in left ventricular non-compaction.\",\"authors\":\"Ladina Erhart, Beat A Kaufmann, Baris Gencer, Philipp K Haager, Hajo Müller, Richard Kobza, Leonhard Held, Simon F Stämpfli\",\"doi\":\"10.5603/CJ.a2022.0105\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>While renal function has been observed to inversely correlate with clinical outcome in other cardiomyopathies, its prognostic significance in patients with left ventricular non-compaction cardiomyopathy (LVNC) has not been investigated. The aim of this study was to determine the prognostic value of renal function in LVNC patients.</p><p><strong>Methods: </strong>Patients with isolated LVNC as diagnosed by echocardiography and/or magnetic resonance imaging in 4 Swiss centers were retrospectively analyzed for this study. Values for creatinine, urea, and estimated glomerular filtration rate (eGFR) as assessed by the CKD-EPI 2009 formula were collected and analyzed by a Cox regression model for the occurrence of a composite endpoint (death or heart transplantation).</p><p><strong>Results: </strong>During the median observation period of 7.4 years 23 patients reached the endpoint. The ageand gender-corrected hazard ratios (HR) for death or heart transplantation were: 1.9 (95% confidence interval [CI] 1.4-2.6) for each increase over baseline creatinine level of 30 μmol/L (p < 0.001), 1.6 (95% CI 1.2-2.2) for each increase over baseline urea level of 5 mmol/L (p = 0.004), and 3.6 (95% CI 1.9-6.9) for each decrease below baseline eGFR level of 30 mL/min (p ≤ 0.001). The HR (log2) for every doubling of creatinine was 7.7 (95% CI 3-19.8; p < 0.001), for every doubling of urea 2.5 (95% CI 1.5-4.3; p < 0.001), and for every bisection of eGFR 5.3 (95% CI 2.4-11.6; p < 0.001).</p><p><strong>Conclusions: </strong>This study provides evidence that in patients with LVNC impairment in renal function is associated with an increased risk of death and heart transplantation suggesting that kidney function assessment should be standard in risk assessment of LVNC patients.</p>\",\"PeriodicalId\":2,\"journal\":{\"name\":\"ACS Applied Bio Materials\",\"volume\":\" \",\"pages\":\"781-789\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10635721/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ACS Applied Bio Materials\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5603/CJ.a2022.0105\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/11/17 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"MATERIALS SCIENCE, BIOMATERIALS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACS Applied Bio Materials","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5603/CJ.a2022.0105","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/11/17 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"MATERIALS SCIENCE, BIOMATERIALS","Score":null,"Total":0}
Renal dysfunction and outcome in left ventricular non-compaction.
Background: While renal function has been observed to inversely correlate with clinical outcome in other cardiomyopathies, its prognostic significance in patients with left ventricular non-compaction cardiomyopathy (LVNC) has not been investigated. The aim of this study was to determine the prognostic value of renal function in LVNC patients.
Methods: Patients with isolated LVNC as diagnosed by echocardiography and/or magnetic resonance imaging in 4 Swiss centers were retrospectively analyzed for this study. Values for creatinine, urea, and estimated glomerular filtration rate (eGFR) as assessed by the CKD-EPI 2009 formula were collected and analyzed by a Cox regression model for the occurrence of a composite endpoint (death or heart transplantation).
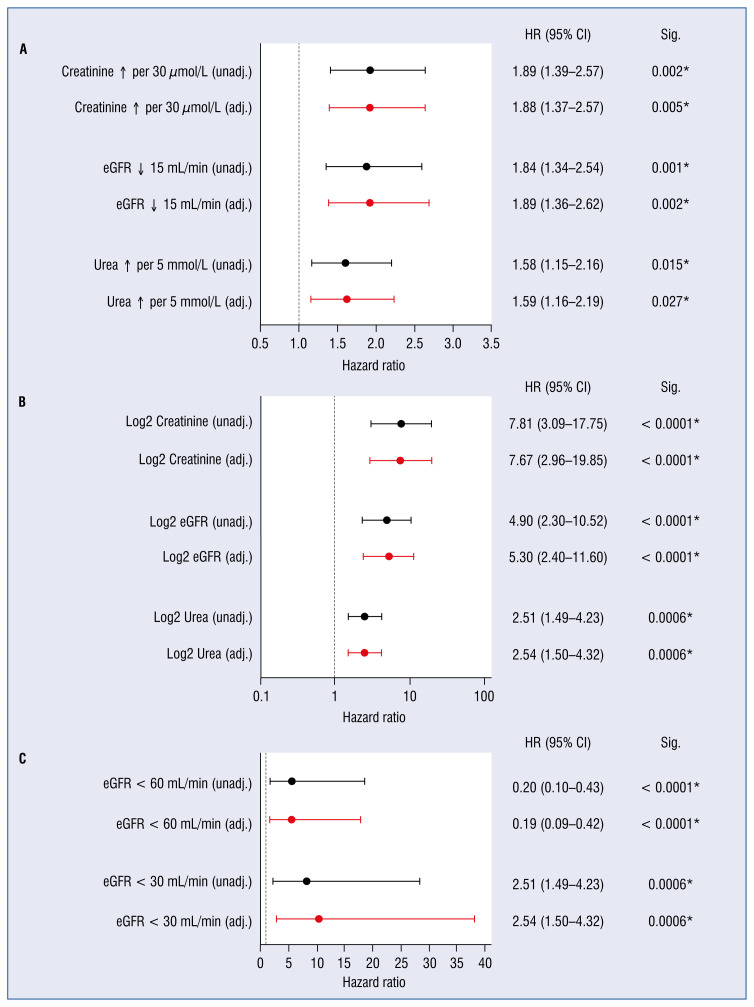
Results: During the median observation period of 7.4 years 23 patients reached the endpoint. The ageand gender-corrected hazard ratios (HR) for death or heart transplantation were: 1.9 (95% confidence interval [CI] 1.4-2.6) for each increase over baseline creatinine level of 30 μmol/L (p < 0.001), 1.6 (95% CI 1.2-2.2) for each increase over baseline urea level of 5 mmol/L (p = 0.004), and 3.6 (95% CI 1.9-6.9) for each decrease below baseline eGFR level of 30 mL/min (p ≤ 0.001). The HR (log2) for every doubling of creatinine was 7.7 (95% CI 3-19.8; p < 0.001), for every doubling of urea 2.5 (95% CI 1.5-4.3; p < 0.001), and for every bisection of eGFR 5.3 (95% CI 2.4-11.6; p < 0.001).
Conclusions: This study provides evidence that in patients with LVNC impairment in renal function is associated with an increased risk of death and heart transplantation suggesting that kidney function assessment should be standard in risk assessment of LVNC patients.
期刊介绍:
ACS Applied Bio Materials is an interdisciplinary journal publishing original research covering all aspects of biomaterials and biointerfaces including and beyond the traditional biosensing, biomedical and therapeutic applications.
The journal is devoted to reports of new and original experimental and theoretical research of an applied nature that integrates knowledge in the areas of materials, engineering, physics, bioscience, and chemistry into important bio applications. The journal is specifically interested in work that addresses the relationship between structure and function and assesses the stability and degradation of materials under relevant environmental and biological conditions.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
