{"title":"肾病咨询可改善急性肾损伤患者的临床结果。","authors":"Harin Rhee, Meeyoung Park, Il Young Kim","doi":"10.23876/j.krcp.23.039","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute kidney injury (AKI) is prevalent in critically ill patients and is associated with an increased risk of in-hospital mortality. Nephrology consultation may be protective, but this has rarely been evaluated in South Korea.</p><p><strong>Methods: </strong>This multicenter retrospective study was based on the electronic medical records (EMRs) of two third-affiliated hospitals. We extracted the records of patients admitted to intensive care units (ICUs) between 2011 and 2020, and retrospectively detected AKI using the modified serum creatinine criteria of the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines. The AKI diagnosis date was defined as the first day of a significant change in serum creatinine level (≥0.3 mg/dL) within 48 hours. Nephrology consultation status was retrieved from the EMRs.</p><p><strong>Results: </strong>In total, 2,461 AKI patients were included; the median age was 65 years (interquartile range [IQR], 56-75 years), 1,459 (59.3%) were male, and 1,065 (43.3%) were of AKI stage 3. During a median of 5 days (IQR, 3-11 days) of ICU admission, nephrology consultations were provided to 512 patients (20.8%). Patients who received such consultations were older, had more comorbidities, and more commonly required dialysis. In a multivariable model, nephrology consultation reduced the risk of in-hospital mortality by 30% (hazard ratio, 0.71; 95% confidence interval, 0.57-0.88). Other factors significant for in-hospital mortality were older age, a higher sequential organ failure assessment (SOFA) score, sepsis, diabetes, hypertension, heart disease, and cancer.</p><p><strong>Conclusion: </strong>For AKI patients in ICUs, nephrology consultation reduced the risk of in-hospital mortality, particularly among those with multiple comorbidities. Therefore, nephrology consultation should not be omitted during ICU care.</p>","PeriodicalId":17716,"journal":{"name":"Kidney Research and Clinical Practice","volume":" ","pages":"102-110"},"PeriodicalIF":3.5000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11838846/pdf/","citationCount":"0","resultStr":"{\"title\":\"Nephrology consultation improves the clinical outcomes of patients with acute kidney injury.\",\"authors\":\"Harin Rhee, Meeyoung Park, Il Young Kim\",\"doi\":\"10.23876/j.krcp.23.039\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Acute kidney injury (AKI) is prevalent in critically ill patients and is associated with an increased risk of in-hospital mortality. Nephrology consultation may be protective, but this has rarely been evaluated in South Korea.</p><p><strong>Methods: </strong>This multicenter retrospective study was based on the electronic medical records (EMRs) of two third-affiliated hospitals. We extracted the records of patients admitted to intensive care units (ICUs) between 2011 and 2020, and retrospectively detected AKI using the modified serum creatinine criteria of the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines. The AKI diagnosis date was defined as the first day of a significant change in serum creatinine level (≥0.3 mg/dL) within 48 hours. Nephrology consultation status was retrieved from the EMRs.</p><p><strong>Results: </strong>In total, 2,461 AKI patients were included; the median age was 65 years (interquartile range [IQR], 56-75 years), 1,459 (59.3%) were male, and 1,065 (43.3%) were of AKI stage 3. During a median of 5 days (IQR, 3-11 days) of ICU admission, nephrology consultations were provided to 512 patients (20.8%). Patients who received such consultations were older, had more comorbidities, and more commonly required dialysis. In a multivariable model, nephrology consultation reduced the risk of in-hospital mortality by 30% (hazard ratio, 0.71; 95% confidence interval, 0.57-0.88). Other factors significant for in-hospital mortality were older age, a higher sequential organ failure assessment (SOFA) score, sepsis, diabetes, hypertension, heart disease, and cancer.</p><p><strong>Conclusion: </strong>For AKI patients in ICUs, nephrology consultation reduced the risk of in-hospital mortality, particularly among those with multiple comorbidities. Therefore, nephrology consultation should not be omitted during ICU care.</p>\",\"PeriodicalId\":17716,\"journal\":{\"name\":\"Kidney Research and Clinical Practice\",\"volume\":\" \",\"pages\":\"102-110\"},\"PeriodicalIF\":3.5000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11838846/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Kidney Research and Clinical Practice\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.23876/j.krcp.23.039\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/9/8 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Kidney Research and Clinical Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.23876/j.krcp.23.039","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/8 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Nephrology consultation improves the clinical outcomes of patients with acute kidney injury.
Background: Acute kidney injury (AKI) is prevalent in critically ill patients and is associated with an increased risk of in-hospital mortality. Nephrology consultation may be protective, but this has rarely been evaluated in South Korea.
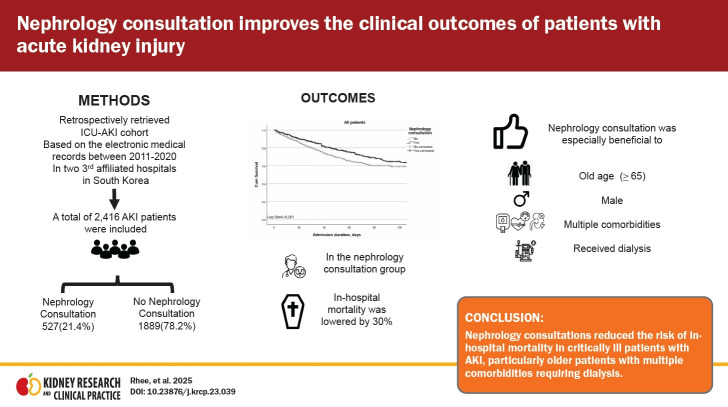
Methods: This multicenter retrospective study was based on the electronic medical records (EMRs) of two third-affiliated hospitals. We extracted the records of patients admitted to intensive care units (ICUs) between 2011 and 2020, and retrospectively detected AKI using the modified serum creatinine criteria of the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines. The AKI diagnosis date was defined as the first day of a significant change in serum creatinine level (≥0.3 mg/dL) within 48 hours. Nephrology consultation status was retrieved from the EMRs.
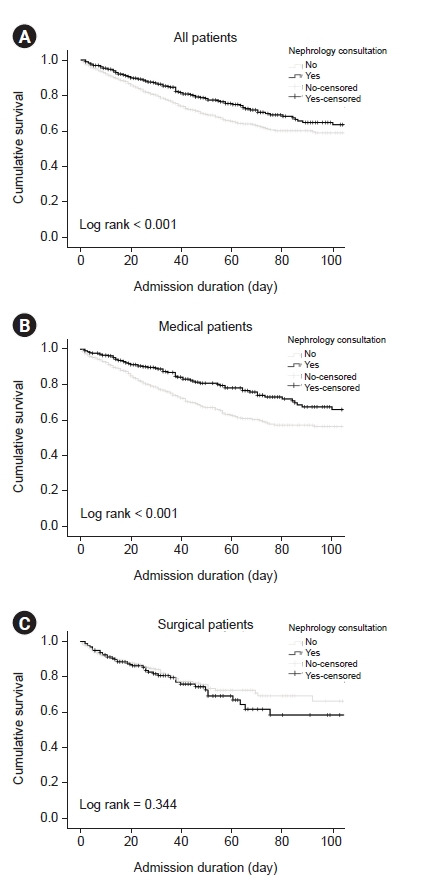
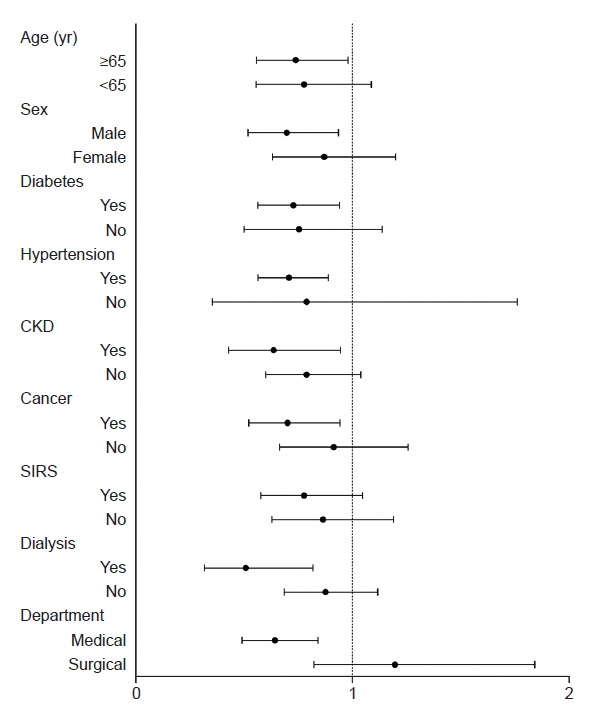
Results: In total, 2,461 AKI patients were included; the median age was 65 years (interquartile range [IQR], 56-75 years), 1,459 (59.3%) were male, and 1,065 (43.3%) were of AKI stage 3. During a median of 5 days (IQR, 3-11 days) of ICU admission, nephrology consultations were provided to 512 patients (20.8%). Patients who received such consultations were older, had more comorbidities, and more commonly required dialysis. In a multivariable model, nephrology consultation reduced the risk of in-hospital mortality by 30% (hazard ratio, 0.71; 95% confidence interval, 0.57-0.88). Other factors significant for in-hospital mortality were older age, a higher sequential organ failure assessment (SOFA) score, sepsis, diabetes, hypertension, heart disease, and cancer.
Conclusion: For AKI patients in ICUs, nephrology consultation reduced the risk of in-hospital mortality, particularly among those with multiple comorbidities. Therefore, nephrology consultation should not be omitted during ICU care.
期刊介绍:
Kidney Research and Clinical Practice (formerly The Korean Journal of Nephrology; ISSN 1975-9460, launched in 1982), the official journal of the Korean Society of Nephrology, is an international, peer-reviewed journal published in English. Its ISO abbreviation is Kidney Res Clin Pract. To provide an efficient venue for dissemination of knowledge and discussion of topics related to basic renal science and clinical practice, the journal offers open access (free submission and free access) and considers articles on all aspects of clinical nephrology and hypertension as well as related molecular genetics, anatomy, pathology, physiology, pharmacology, and immunology. In particular, the journal focuses on translational renal research that helps bridging laboratory discovery with the diagnosis and treatment of human kidney disease. Topics covered include basic science with possible clinical applicability and papers on the pathophysiological basis of disease processes of the kidney. Original researches from areas of intervention nephrology or dialysis access are also welcomed. Major article types considered for publication include original research and reviews on current topics of interest. Accepted manuscripts are granted free online open-access immediately after publication, which permits its users to read, download, copy, distribute, print, search, or link to the full texts of its articles to facilitate access to a broad readership. Circulation number of print copies is 1,600.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
