{"title":"高磷血症家族性肿瘤的老年性钙沉着症高磷血症综合征:硬皮病合并症的作用。","authors":"Hiroaki Iwasaki","doi":"10.1530/EDM-23-0071","DOIUrl":null,"url":null,"abstract":"<p><strong>Summary: </strong>A 73-year-old woman with type 2 diabetes mellitus was referred to our department for glycaemic control. Physical examination revealed two subcutaneous hard masses around the left shoulder and the right hip joint. The patient could not fully extend her fingers because of skin sclerosis in both hands. Laboratory studies showed hyperphosphataemia and a high ratio of renal tubular maximum reabsorption of phosphate to glomerular filtration rate. There were no abnormalities in serum calcium, creatinine, alkaline phosphatase, and intact parathyroid hormone levels, whereas serum fibroblast growth factor 23 was low. Hyperphosphataemic familial tumoural calcinosis/hyperostosis-hyperphosphataemia syndrome (HFTC/HHS) was diagnosed using whole genome sequencing that revealed a novel frameshift beyond the 584th threonine located in the lectin domain of UDP-N-acetyl-alpha-D-galactosamine:polypeptide N-acetylgalactosaminyltransferase 3 associated with a duplication of the 1748th thymine in the coding region of the corresponding gene. Furthermore, anti-nuclear, anti-centromere, and anti-cardiolipin antibodies were positive, implying that comorbid limited type scleroderma might play a role in tumoural calcinosis (TC) development. A low phosphate diet was prescribed with phosphate-lowering medications, including aluminium hydroxide, acetazolamide, and sevelamer hydrochloride. The patient displayed a decrease in serum phosphate levels from 6.5 to 5.5 mg/dL 10 months after the initiation of treatment, but her TC had not improved during treatment for more than 1 year. This case was interesting because the patient with HFTC/HHS exhibited TC despite being over her 60s, and subsequent scleroderma might contribute to the specific clinical course. When HFTC/HHS presents with elderly-onset TC, the involvement of comorbidities in exacerbating TC should be considered.</p><p><strong>Learning points: </strong>HFTC/HHS occurs on an autosomal recessive basis, but its clinical course and manifestations differ significantly throughout the cases. HFTC/HHS may be undiagnosed until later in life because of its rarity, unfamiliarity, and phenotype diversity; therefore, HFTC/HHS should be included in the differential diagnosis of elderly patients with unexplained hyperphosphataemia or ectopic calcinosis. Comorbidities, including rheumatologic disorders, may contribute to developing HFTC/HHS-associated calcinosis.</p>","PeriodicalId":37467,"journal":{"name":"Endocrinology, Diabetes and Metabolism Case Reports","volume":"2023 4","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2023-10-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/aa/d0/EDM23-0071.PMC10563600.pdf","citationCount":"0","resultStr":"{\"title\":\"Elderly-onset calcinosis of hyperphosphataemic familial tumoural calcinosis/hyperostosis-hyperphosphataemia syndrome: the role of comorbid scleroderma.\",\"authors\":\"Hiroaki Iwasaki\",\"doi\":\"10.1530/EDM-23-0071\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Summary: </strong>A 73-year-old woman with type 2 diabetes mellitus was referred to our department for glycaemic control. Physical examination revealed two subcutaneous hard masses around the left shoulder and the right hip joint. The patient could not fully extend her fingers because of skin sclerosis in both hands. Laboratory studies showed hyperphosphataemia and a high ratio of renal tubular maximum reabsorption of phosphate to glomerular filtration rate. There were no abnormalities in serum calcium, creatinine, alkaline phosphatase, and intact parathyroid hormone levels, whereas serum fibroblast growth factor 23 was low. Hyperphosphataemic familial tumoural calcinosis/hyperostosis-hyperphosphataemia syndrome (HFTC/HHS) was diagnosed using whole genome sequencing that revealed a novel frameshift beyond the 584th threonine located in the lectin domain of UDP-N-acetyl-alpha-D-galactosamine:polypeptide N-acetylgalactosaminyltransferase 3 associated with a duplication of the 1748th thymine in the coding region of the corresponding gene. Furthermore, anti-nuclear, anti-centromere, and anti-cardiolipin antibodies were positive, implying that comorbid limited type scleroderma might play a role in tumoural calcinosis (TC) development. A low phosphate diet was prescribed with phosphate-lowering medications, including aluminium hydroxide, acetazolamide, and sevelamer hydrochloride. The patient displayed a decrease in serum phosphate levels from 6.5 to 5.5 mg/dL 10 months after the initiation of treatment, but her TC had not improved during treatment for more than 1 year. This case was interesting because the patient with HFTC/HHS exhibited TC despite being over her 60s, and subsequent scleroderma might contribute to the specific clinical course. When HFTC/HHS presents with elderly-onset TC, the involvement of comorbidities in exacerbating TC should be considered.</p><p><strong>Learning points: </strong>HFTC/HHS occurs on an autosomal recessive basis, but its clinical course and manifestations differ significantly throughout the cases. HFTC/HHS may be undiagnosed until later in life because of its rarity, unfamiliarity, and phenotype diversity; therefore, HFTC/HHS should be included in the differential diagnosis of elderly patients with unexplained hyperphosphataemia or ectopic calcinosis. Comorbidities, including rheumatologic disorders, may contribute to developing HFTC/HHS-associated calcinosis.</p>\",\"PeriodicalId\":37467,\"journal\":{\"name\":\"Endocrinology, Diabetes and Metabolism Case Reports\",\"volume\":\"2023 4\",\"pages\":\"\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2023-10-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/aa/d0/EDM23-0071.PMC10563600.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Endocrinology, Diabetes and Metabolism Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1530/EDM-23-0071\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/10/1 0:00:00\",\"PubModel\":\"Print\",\"JCR\":\"Q4\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrinology, Diabetes and Metabolism Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EDM-23-0071","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/1 0:00:00","PubModel":"Print","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Elderly-onset calcinosis of hyperphosphataemic familial tumoural calcinosis/hyperostosis-hyperphosphataemia syndrome: the role of comorbid scleroderma.
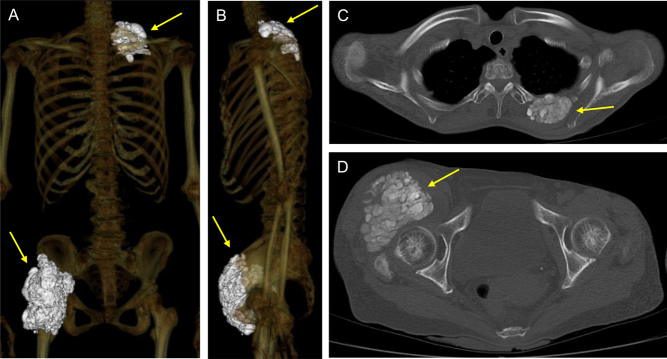
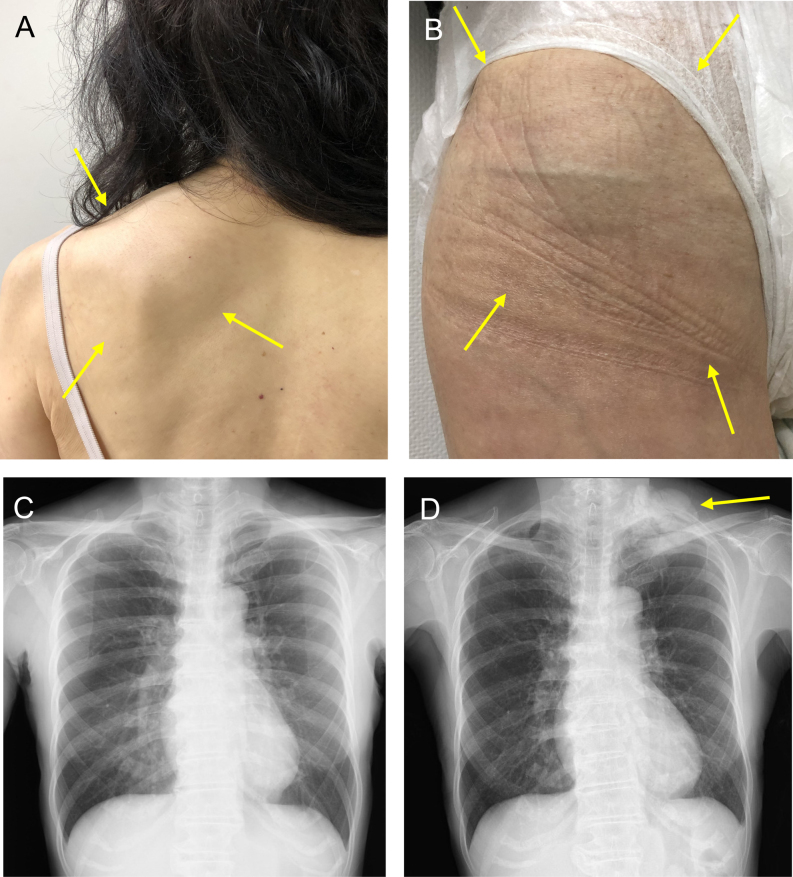
Summary: A 73-year-old woman with type 2 diabetes mellitus was referred to our department for glycaemic control. Physical examination revealed two subcutaneous hard masses around the left shoulder and the right hip joint. The patient could not fully extend her fingers because of skin sclerosis in both hands. Laboratory studies showed hyperphosphataemia and a high ratio of renal tubular maximum reabsorption of phosphate to glomerular filtration rate. There were no abnormalities in serum calcium, creatinine, alkaline phosphatase, and intact parathyroid hormone levels, whereas serum fibroblast growth factor 23 was low. Hyperphosphataemic familial tumoural calcinosis/hyperostosis-hyperphosphataemia syndrome (HFTC/HHS) was diagnosed using whole genome sequencing that revealed a novel frameshift beyond the 584th threonine located in the lectin domain of UDP-N-acetyl-alpha-D-galactosamine:polypeptide N-acetylgalactosaminyltransferase 3 associated with a duplication of the 1748th thymine in the coding region of the corresponding gene. Furthermore, anti-nuclear, anti-centromere, and anti-cardiolipin antibodies were positive, implying that comorbid limited type scleroderma might play a role in tumoural calcinosis (TC) development. A low phosphate diet was prescribed with phosphate-lowering medications, including aluminium hydroxide, acetazolamide, and sevelamer hydrochloride. The patient displayed a decrease in serum phosphate levels from 6.5 to 5.5 mg/dL 10 months after the initiation of treatment, but her TC had not improved during treatment for more than 1 year. This case was interesting because the patient with HFTC/HHS exhibited TC despite being over her 60s, and subsequent scleroderma might contribute to the specific clinical course. When HFTC/HHS presents with elderly-onset TC, the involvement of comorbidities in exacerbating TC should be considered.
Learning points: HFTC/HHS occurs on an autosomal recessive basis, but its clinical course and manifestations differ significantly throughout the cases. HFTC/HHS may be undiagnosed until later in life because of its rarity, unfamiliarity, and phenotype diversity; therefore, HFTC/HHS should be included in the differential diagnosis of elderly patients with unexplained hyperphosphataemia or ectopic calcinosis. Comorbidities, including rheumatologic disorders, may contribute to developing HFTC/HHS-associated calcinosis.
期刊介绍:
Endocrinology, Diabetes & Metabolism Case Reports publishes case reports on common and rare conditions in all areas of clinical endocrinology, diabetes and metabolism. Articles should include clear learning points which readers can use to inform medical education or clinical practice. The types of cases of interest to Endocrinology, Diabetes & Metabolism Case Reports include: -Insight into disease pathogenesis or mechanism of therapy - Novel diagnostic procedure - Novel treatment - Unique/unexpected symptoms or presentations of a disease - New disease or syndrome: presentations/diagnosis/management - Unusual effects of medical treatment - Error in diagnosis/pitfalls and caveats




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
