{"title":"无心绞痛患者主要心血管不良事件的十年预测因素。","authors":"Preesha Premsagar, Colleen Aldous, Tonya Esterhuizen","doi":"10.4102/safp.v65i1.5629","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Longstanding cardiovascular risk factors cause major adverse cardiovascular events (MACE). Major adverse cardiovascular events prediction may improve outcomes. The aim was to evaluate the ten-year predictors of MACE in patients without angina.</p><p><strong>Methods: </strong>Patients referred to Inkosi Albert Luthuli Hospital, Durban, South Africa, without typical angina from 2002 to 2008 were collected and followed up for MACE from 2009 to 2019. Survival time was calculated in months. Independent variables were tested with Cox proportional hazard models to predict MACE morbidity and MACE mortality.</p><p><strong>Results: </strong>There were 525 patients; 401 (76.0%) were Indian, 167 (31.8%) had diabetes at baseline. At 10-year follow up 157/525 (29.9%) experienced MACE morbidity, of whom, 82/525 (15.6%) had MACE mortality. There were 368/525 (70.1%) patients censored, of whom 195/525 (37.1%) were lost to follow up. For MACE morbidity, mean and longest observation times were 102.2 and 201 months, respectively. Predictors for MACE morbidity were age (hazard ratio [HR] = 1.025), diabetes (HR = 1.436), Duke Risk category (HR = 1.562) and Ischaemic burden category (HR = 1.531). For MACE mortality, mean and longest observation times were 107.9 and 204 months, respectively. Predictors for MACE mortality were age (HR = 1.044), Duke Risk category (HR = 1.983), echocardiography risk category (HR = 2.537) and Ischaemic burden category (HR = 1.780).</p><p><strong>Conclusion: </strong>Among patients without typical angina, early ischaemia on noninvasive tests indicated microvascular disease and hyperglycaemia, predicting long-term MACE morbidity and MACE mortality.Contribution: Diabetes was a predictor for MACE morbidity but not for MACE mortality; patients lost to follow-up were possibly diabetic patients with MACE mortality at district hospitals. Early screening for ischaemia and hyperglycaemia control may improve outcomes.</p>","PeriodicalId":22040,"journal":{"name":"South African Family Practice","volume":"65 1","pages":"e1-e9"},"PeriodicalIF":1.4000,"publicationDate":"2023-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10476236/pdf/","citationCount":"0","resultStr":"{\"title\":\"Ten-year predictors of major adverse cardiovascular events in patients without angina.\",\"authors\":\"Preesha Premsagar, Colleen Aldous, Tonya Esterhuizen\",\"doi\":\"10.4102/safp.v65i1.5629\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Longstanding cardiovascular risk factors cause major adverse cardiovascular events (MACE). Major adverse cardiovascular events prediction may improve outcomes. The aim was to evaluate the ten-year predictors of MACE in patients without angina.</p><p><strong>Methods: </strong>Patients referred to Inkosi Albert Luthuli Hospital, Durban, South Africa, without typical angina from 2002 to 2008 were collected and followed up for MACE from 2009 to 2019. Survival time was calculated in months. Independent variables were tested with Cox proportional hazard models to predict MACE morbidity and MACE mortality.</p><p><strong>Results: </strong>There were 525 patients; 401 (76.0%) were Indian, 167 (31.8%) had diabetes at baseline. At 10-year follow up 157/525 (29.9%) experienced MACE morbidity, of whom, 82/525 (15.6%) had MACE mortality. There were 368/525 (70.1%) patients censored, of whom 195/525 (37.1%) were lost to follow up. For MACE morbidity, mean and longest observation times were 102.2 and 201 months, respectively. Predictors for MACE morbidity were age (hazard ratio [HR] = 1.025), diabetes (HR = 1.436), Duke Risk category (HR = 1.562) and Ischaemic burden category (HR = 1.531). For MACE mortality, mean and longest observation times were 107.9 and 204 months, respectively. Predictors for MACE mortality were age (HR = 1.044), Duke Risk category (HR = 1.983), echocardiography risk category (HR = 2.537) and Ischaemic burden category (HR = 1.780).</p><p><strong>Conclusion: </strong>Among patients without typical angina, early ischaemia on noninvasive tests indicated microvascular disease and hyperglycaemia, predicting long-term MACE morbidity and MACE mortality.Contribution: Diabetes was a predictor for MACE morbidity but not for MACE mortality; patients lost to follow-up were possibly diabetic patients with MACE mortality at district hospitals. Early screening for ischaemia and hyperglycaemia control may improve outcomes.</p>\",\"PeriodicalId\":22040,\"journal\":{\"name\":\"South African Family Practice\",\"volume\":\"65 1\",\"pages\":\"e1-e9\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2023-08-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10476236/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"South African Family Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4102/safp.v65i1.5629\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"South African Family Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4102/safp.v65i1.5629","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
背景:长期存在的心血管危险因素会导致重大心血管不良事件(MACE)。重大心血管不良事件的预测可能会改善预后。目的是评估无心绞痛患者MACE的十年预测因素。方法:收集2002年至2008年在南非德班Inkosi Albert Luthuli医院就诊的无典型心绞痛患者,并于2009年至2019年对其进行MACE随访。存活时间以月为单位计算。用Cox比例风险模型检验自变量,预测MACE发病率和死亡率。结果:525例;401人(76.0%)是印度人,167人(31.8%)在基线时患有糖尿病。在10年的随访中,157/525(29.9%)经历了MACE发病率,其中82/525(15.6%)有MACE死亡率。共有368/525名(70.1%)患者接受了审查,其中195/525(37.1%)患者失去了随访。MACE发病率的平均观察时间和最长观察时间分别为102.2个月和201个月。MACE发病率的预测因素为年龄(危险比[HR]=1.025)、糖尿病(HR=1.436)、杜克风险类别(HR=1.562)和缺血性负荷类别(HR1.531)。MACE死亡率的平均观察时间和最长观察时间分别为107.9个月和204个月。MACE死亡率的预测因素为年龄(HR=1.044)、杜克风险类别(HR=1.983)、超声心动图风险类别(HR=2.537)和缺血性负荷类别(HR=1.780)。贡献:糖尿病是MACE发病率的预测因素,但不是MACE死亡率的预测因素;失去随访的患者可能是地区医院的糖尿病患者,MACE死亡率较高。早期筛查缺血和高血糖控制可能会改善预后。
Ten-year predictors of major adverse cardiovascular events in patients without angina.
Background: Longstanding cardiovascular risk factors cause major adverse cardiovascular events (MACE). Major adverse cardiovascular events prediction may improve outcomes. The aim was to evaluate the ten-year predictors of MACE in patients without angina.
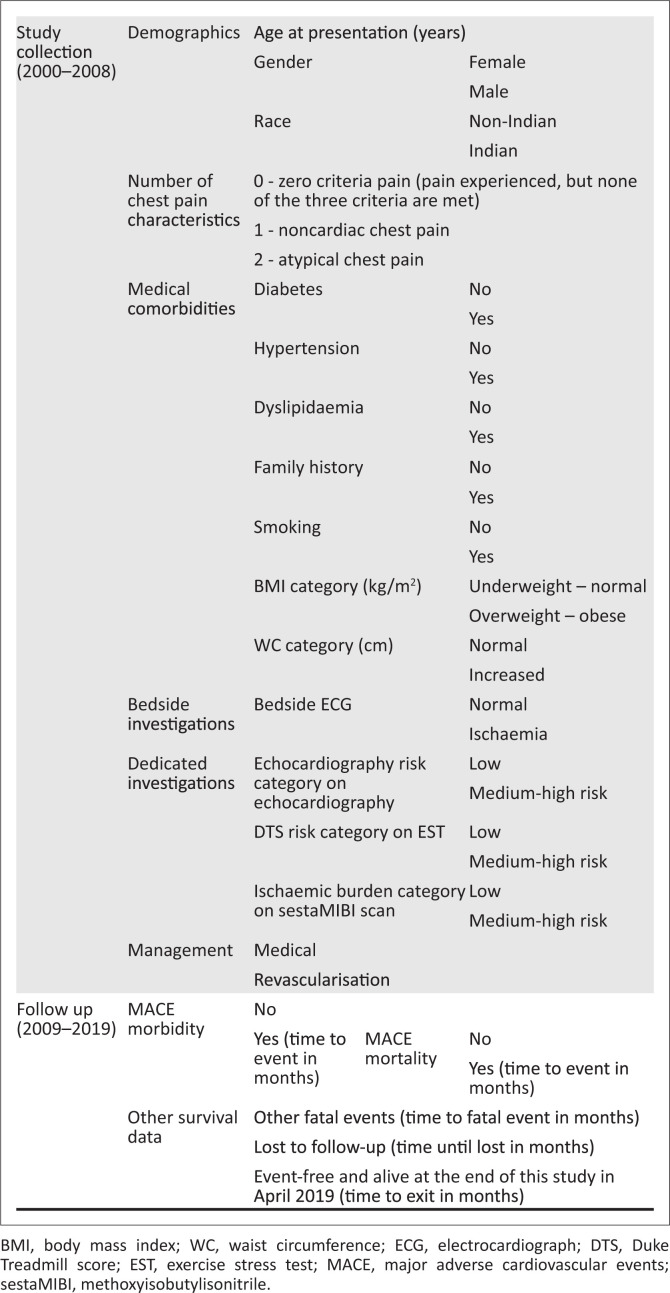
Methods: Patients referred to Inkosi Albert Luthuli Hospital, Durban, South Africa, without typical angina from 2002 to 2008 were collected and followed up for MACE from 2009 to 2019. Survival time was calculated in months. Independent variables were tested with Cox proportional hazard models to predict MACE morbidity and MACE mortality.
Results: There were 525 patients; 401 (76.0%) were Indian, 167 (31.8%) had diabetes at baseline. At 10-year follow up 157/525 (29.9%) experienced MACE morbidity, of whom, 82/525 (15.6%) had MACE mortality. There were 368/525 (70.1%) patients censored, of whom 195/525 (37.1%) were lost to follow up. For MACE morbidity, mean and longest observation times were 102.2 and 201 months, respectively. Predictors for MACE morbidity were age (hazard ratio [HR] = 1.025), diabetes (HR = 1.436), Duke Risk category (HR = 1.562) and Ischaemic burden category (HR = 1.531). For MACE mortality, mean and longest observation times were 107.9 and 204 months, respectively. Predictors for MACE mortality were age (HR = 1.044), Duke Risk category (HR = 1.983), echocardiography risk category (HR = 2.537) and Ischaemic burden category (HR = 1.780).
Conclusion: Among patients without typical angina, early ischaemia on noninvasive tests indicated microvascular disease and hyperglycaemia, predicting long-term MACE morbidity and MACE mortality.Contribution: Diabetes was a predictor for MACE morbidity but not for MACE mortality; patients lost to follow-up were possibly diabetic patients with MACE mortality at district hospitals. Early screening for ischaemia and hyperglycaemia control may improve outcomes.
期刊介绍:
South African Family Practice (SAFP) is a peer-reviewed scientific journal, which strives to provide primary care physicians and researchers with a broad range of scholarly work in the disciplines of Family Medicine, Primary Health Care, Rural Medicine, District Health and other related fields. SAFP publishes original research, clinical reviews, and pertinent commentary that advance the knowledge base of these disciplines. The content of SAFP is designed to reflect and support further development of the broad basis of these disciplines through original research and critical review of evidence in important clinical areas; as well as to provide practitioners with continuing professional development material.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
