Shahla Siddiqui, Diana Bouhassira, Lauren Kelly, Margaret Hayes, Austin Herbst, Sarah Ohnigian, Luke Hedrick, Kimberly Ona Ayala, Daniel S Talmor, Jennifer P Stevens
{"title":"检查种族在重症监护室临终关怀中的作用:一项单中心观察研究。","authors":"Shahla Siddiqui, Diana Bouhassira, Lauren Kelly, Margaret Hayes, Austin Herbst, Sarah Ohnigian, Luke Hedrick, Kimberly Ona Ayala, Daniel S Talmor, Jennifer P Stevens","doi":"10.1089/pmr.2023.0037","DOIUrl":null,"url":null,"abstract":"Background: Prior studies have shown variation in the intensity of end-of-life care in intensive care units (ICUs) among patients of different races. Objective: We sought to identify variation in the levels of care at the end of life in the ICU and to assess for any association with race and ethnicity. Design: An observational, retrospective cohort study. Settings: A tertiary care center in Boston, MA. Participants: All critically ill patients admitted to medical and surgical ICUs between June 2019 and December 2020. Exposure: Self-identified race and ethnicity. Main Outcome and Measure: The primary outcome was death. Secondary outcomes included “code status,” markers of intensity of care, consultation by the Palliative care service, and consultation by the Ethics service. Results: A total of 9083 ICU patient encounters were analyzed. One thousand two hundred fifty-nine patients (14%) died in the ICU; the mean age of patients was 64 years (standard deviation 16.8), and 44% of patients were women. A large number of decedents (22.7%) did not have their race identified. These patients had a high rate of interventions at death. Code status varied by race, with more White patients designated as “Comfort Measures Only” (CMO) (74%) whereas more Black patients were designated as “Do Not Resuscitate/Do Not Intubate (DNR/DNI) and DNR/ok to intubate” (12.1% and 15.7%) at the end of life; after adjustment for age and severity of illness, there were no statistical differences by race for the use of the CMO code status. Use of dialysis at the end of life varied by self-identified race. Specifically, Black and Unknown patients were more likely to receive renal replacement therapy, even after adjustment for age and severity of illness (24% and 20%, p = 0.003). Conclusions: Our data describe a gap in identification of race and ethnicity, as well as differences at the end of life in the ICU, especially with respect to code status and certain markers of intensity.","PeriodicalId":74394,"journal":{"name":"Palliative medicine reports","volume":"4 1","pages":"264-273"},"PeriodicalIF":1.3000,"publicationDate":"2023-09-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10507941/pdf/","citationCount":"0","resultStr":"{\"title\":\"Examining the Role of Race in End-of-Life Care in the Intensive Care Unit: A Single-Center Observational Study.\",\"authors\":\"Shahla Siddiqui, Diana Bouhassira, Lauren Kelly, Margaret Hayes, Austin Herbst, Sarah Ohnigian, Luke Hedrick, Kimberly Ona Ayala, Daniel S Talmor, Jennifer P Stevens\",\"doi\":\"10.1089/pmr.2023.0037\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Background: Prior studies have shown variation in the intensity of end-of-life care in intensive care units (ICUs) among patients of different races. Objective: We sought to identify variation in the levels of care at the end of life in the ICU and to assess for any association with race and ethnicity. Design: An observational, retrospective cohort study. Settings: A tertiary care center in Boston, MA. Participants: All critically ill patients admitted to medical and surgical ICUs between June 2019 and December 2020. Exposure: Self-identified race and ethnicity. Main Outcome and Measure: The primary outcome was death. Secondary outcomes included “code status,” markers of intensity of care, consultation by the Palliative care service, and consultation by the Ethics service. Results: A total of 9083 ICU patient encounters were analyzed. One thousand two hundred fifty-nine patients (14%) died in the ICU; the mean age of patients was 64 years (standard deviation 16.8), and 44% of patients were women. A large number of decedents (22.7%) did not have their race identified. These patients had a high rate of interventions at death. Code status varied by race, with more White patients designated as “Comfort Measures Only” (CMO) (74%) whereas more Black patients were designated as “Do Not Resuscitate/Do Not Intubate (DNR/DNI) and DNR/ok to intubate” (12.1% and 15.7%) at the end of life; after adjustment for age and severity of illness, there were no statistical differences by race for the use of the CMO code status. Use of dialysis at the end of life varied by self-identified race. Specifically, Black and Unknown patients were more likely to receive renal replacement therapy, even after adjustment for age and severity of illness (24% and 20%, p = 0.003). Conclusions: Our data describe a gap in identification of race and ethnicity, as well as differences at the end of life in the ICU, especially with respect to code status and certain markers of intensity.\",\"PeriodicalId\":74394,\"journal\":{\"name\":\"Palliative medicine reports\",\"volume\":\"4 1\",\"pages\":\"264-273\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2023-09-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10507941/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Palliative medicine reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1089/pmr.2023.0037\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Palliative medicine reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/pmr.2023.0037","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Examining the Role of Race in End-of-Life Care in the Intensive Care Unit: A Single-Center Observational Study.
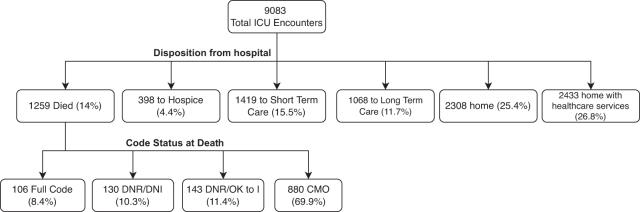
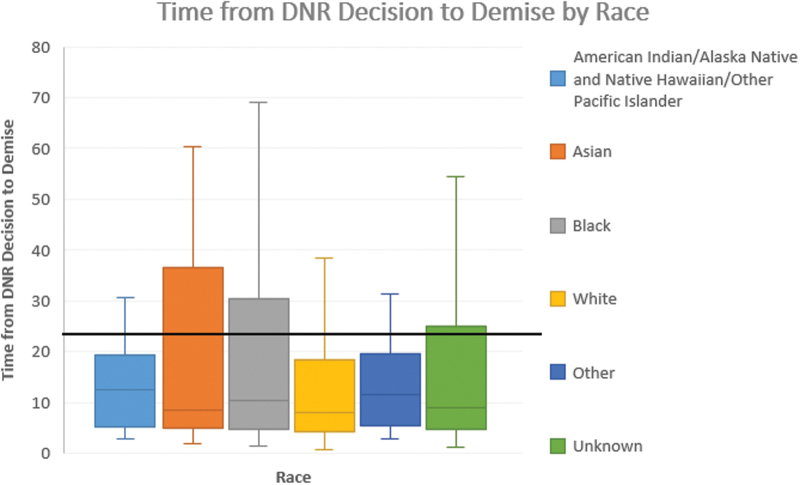
Background: Prior studies have shown variation in the intensity of end-of-life care in intensive care units (ICUs) among patients of different races. Objective: We sought to identify variation in the levels of care at the end of life in the ICU and to assess for any association with race and ethnicity. Design: An observational, retrospective cohort study. Settings: A tertiary care center in Boston, MA. Participants: All critically ill patients admitted to medical and surgical ICUs between June 2019 and December 2020. Exposure: Self-identified race and ethnicity. Main Outcome and Measure: The primary outcome was death. Secondary outcomes included “code status,” markers of intensity of care, consultation by the Palliative care service, and consultation by the Ethics service. Results: A total of 9083 ICU patient encounters were analyzed. One thousand two hundred fifty-nine patients (14%) died in the ICU; the mean age of patients was 64 years (standard deviation 16.8), and 44% of patients were women. A large number of decedents (22.7%) did not have their race identified. These patients had a high rate of interventions at death. Code status varied by race, with more White patients designated as “Comfort Measures Only” (CMO) (74%) whereas more Black patients were designated as “Do Not Resuscitate/Do Not Intubate (DNR/DNI) and DNR/ok to intubate” (12.1% and 15.7%) at the end of life; after adjustment for age and severity of illness, there were no statistical differences by race for the use of the CMO code status. Use of dialysis at the end of life varied by self-identified race. Specifically, Black and Unknown patients were more likely to receive renal replacement therapy, even after adjustment for age and severity of illness (24% and 20%, p = 0.003). Conclusions: Our data describe a gap in identification of race and ethnicity, as well as differences at the end of life in the ICU, especially with respect to code status and certain markers of intensity.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
