Sara Mohammed, João Matos, Matthieu Doutreligne, Leo Anthony Celi, Tristan Struja
{"title":"败血症患者侵入性ICU治疗中的种族差异:来自MIMIC-IV的高分辨率电子健康记录分析。","authors":"Sara Mohammed, João Matos, Matthieu Doutreligne, Leo Anthony Celi, Tristan Struja","doi":"10.59249/WDJI8829","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b>: Low-resolution administrative databases can give biased results, whereas high-resolution, time-stamped variables from clinical databases like MIMIC-IV might provide nuanced insights. We evaluated racial-ethnic disparities in life-sustaining ICU-treatments (Invasive Mechanical Ventilation (IMV), Renal Replacement Therapy (RRT), and Vasopressors (VP)) among patients with sepsis. <b>Methods</b>: In this observational retrospective cohort study, patients fulfilling sepsis-3 criteria were categorized by treatment assignment within the first 4 days. The outcomes were treatment allocations. The likelihood of receiving treatment was calculated by race-ethnicity (Racial-ethnic group (REG) or White group (WG)) using 5-fold sub-sampling nested logistic regression and XGBoost. <b>Results</b>: In 23,914 admissions, 82% were White, 42% were women. REG were less likely to receive IMV across all eligibility days (day 1 odds ratio (OR) 0.87, 95% confidence interval (CI) 0.83-0.94, day 4 OR 0.80, 95% CI 0.72 - 0.87). There were no differences in RRT (day 1 OR 1.00, 95% CI 0.96-1.09, day 4 OR 1.00, 95% CI 0.94-1.06). REG were also less likely to be treated with VP at days 1 to 3 (day 1 OR 0.87, 95% CI 0.76-0.94), but not at day 4 (OR 0.95, 95% CI 0.87-1.01). These findings remained robust when relaxing eligibility criteria for treatment allocation. <b>Conclusion</b>: Our findings reveal significant disparities in the use of invasive life-saving ICU treatments among septic patients from racial and ethnic minority backgrounds, particularly with respect to IMV and VP use. These disparities underscore not only the need to address inequality in critical care settings, but also highlight the importance of high-resolution data.</p>","PeriodicalId":48617,"journal":{"name":"Yale Journal of Biology and Medicine","volume":"96 3","pages":"293-312"},"PeriodicalIF":3.9000,"publicationDate":"2023-09-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/78/ba/yjbm_96_3_293.PMC10524813.pdf","citationCount":"0","resultStr":"{\"title\":\"Racial Disparities in Invasive ICU Treatments Among Septic Patients: High Resolution Electronic Health Records Analysis from MIMIC-IV.\",\"authors\":\"Sara Mohammed, João Matos, Matthieu Doutreligne, Leo Anthony Celi, Tristan Struja\",\"doi\":\"10.59249/WDJI8829\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background</b>: Low-resolution administrative databases can give biased results, whereas high-resolution, time-stamped variables from clinical databases like MIMIC-IV might provide nuanced insights. We evaluated racial-ethnic disparities in life-sustaining ICU-treatments (Invasive Mechanical Ventilation (IMV), Renal Replacement Therapy (RRT), and Vasopressors (VP)) among patients with sepsis. <b>Methods</b>: In this observational retrospective cohort study, patients fulfilling sepsis-3 criteria were categorized by treatment assignment within the first 4 days. The outcomes were treatment allocations. The likelihood of receiving treatment was calculated by race-ethnicity (Racial-ethnic group (REG) or White group (WG)) using 5-fold sub-sampling nested logistic regression and XGBoost. <b>Results</b>: In 23,914 admissions, 82% were White, 42% were women. REG were less likely to receive IMV across all eligibility days (day 1 odds ratio (OR) 0.87, 95% confidence interval (CI) 0.83-0.94, day 4 OR 0.80, 95% CI 0.72 - 0.87). There were no differences in RRT (day 1 OR 1.00, 95% CI 0.96-1.09, day 4 OR 1.00, 95% CI 0.94-1.06). REG were also less likely to be treated with VP at days 1 to 3 (day 1 OR 0.87, 95% CI 0.76-0.94), but not at day 4 (OR 0.95, 95% CI 0.87-1.01). These findings remained robust when relaxing eligibility criteria for treatment allocation. <b>Conclusion</b>: Our findings reveal significant disparities in the use of invasive life-saving ICU treatments among septic patients from racial and ethnic minority backgrounds, particularly with respect to IMV and VP use. These disparities underscore not only the need to address inequality in critical care settings, but also highlight the importance of high-resolution data.</p>\",\"PeriodicalId\":48617,\"journal\":{\"name\":\"Yale Journal of Biology and Medicine\",\"volume\":\"96 3\",\"pages\":\"293-312\"},\"PeriodicalIF\":3.9000,\"publicationDate\":\"2023-09-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/78/ba/yjbm_96_3_293.PMC10524813.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Yale Journal of Biology and Medicine\",\"FirstCategoryId\":\"5\",\"ListUrlMain\":\"https://doi.org/10.59249/WDJI8829\",\"RegionNum\":3,\"RegionCategory\":\"工程技术\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"BIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Yale Journal of Biology and Medicine","FirstCategoryId":"5","ListUrlMain":"https://doi.org/10.59249/WDJI8829","RegionNum":3,"RegionCategory":"工程技术","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"BIOLOGY","Score":null,"Total":0}
Racial Disparities in Invasive ICU Treatments Among Septic Patients: High Resolution Electronic Health Records Analysis from MIMIC-IV.
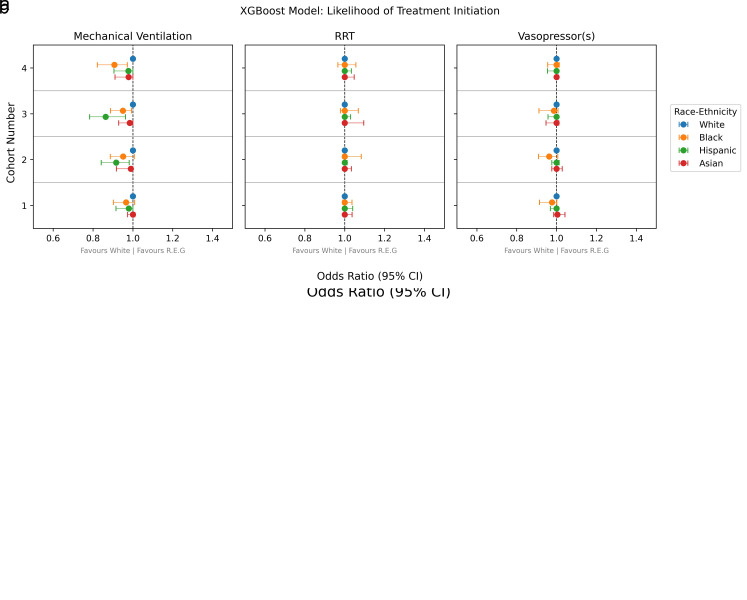
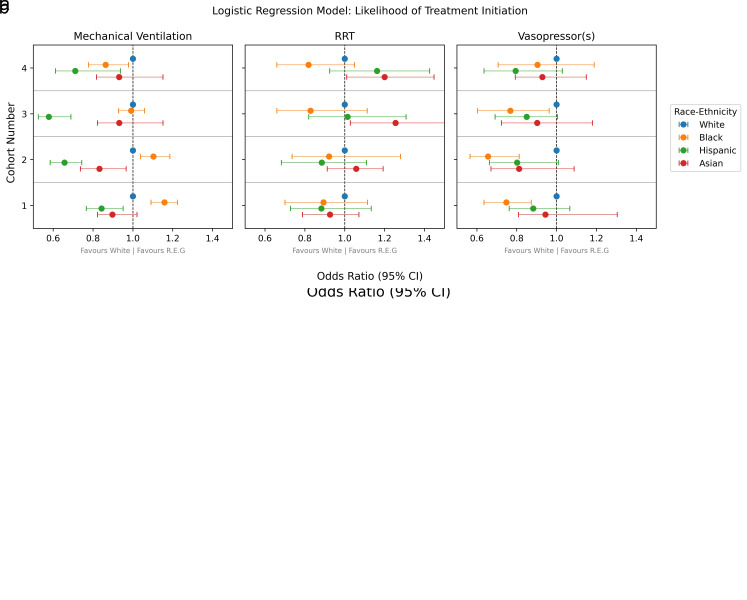
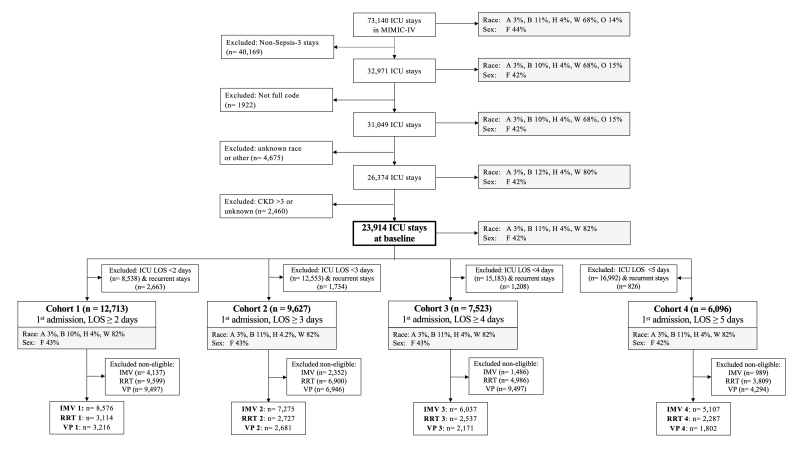
Background: Low-resolution administrative databases can give biased results, whereas high-resolution, time-stamped variables from clinical databases like MIMIC-IV might provide nuanced insights. We evaluated racial-ethnic disparities in life-sustaining ICU-treatments (Invasive Mechanical Ventilation (IMV), Renal Replacement Therapy (RRT), and Vasopressors (VP)) among patients with sepsis. Methods: In this observational retrospective cohort study, patients fulfilling sepsis-3 criteria were categorized by treatment assignment within the first 4 days. The outcomes were treatment allocations. The likelihood of receiving treatment was calculated by race-ethnicity (Racial-ethnic group (REG) or White group (WG)) using 5-fold sub-sampling nested logistic regression and XGBoost. Results: In 23,914 admissions, 82% were White, 42% were women. REG were less likely to receive IMV across all eligibility days (day 1 odds ratio (OR) 0.87, 95% confidence interval (CI) 0.83-0.94, day 4 OR 0.80, 95% CI 0.72 - 0.87). There were no differences in RRT (day 1 OR 1.00, 95% CI 0.96-1.09, day 4 OR 1.00, 95% CI 0.94-1.06). REG were also less likely to be treated with VP at days 1 to 3 (day 1 OR 0.87, 95% CI 0.76-0.94), but not at day 4 (OR 0.95, 95% CI 0.87-1.01). These findings remained robust when relaxing eligibility criteria for treatment allocation. Conclusion: Our findings reveal significant disparities in the use of invasive life-saving ICU treatments among septic patients from racial and ethnic minority backgrounds, particularly with respect to IMV and VP use. These disparities underscore not only the need to address inequality in critical care settings, but also highlight the importance of high-resolution data.
期刊介绍:
The Yale Journal of Biology and Medicine (YJBM) is a graduate and medical student-run, peer-reviewed, open-access journal dedicated to the publication of original research articles, scientific reviews, articles on medical history, personal perspectives on medicine, policy analyses, case reports, and symposia related to biomedical matters. YJBM is published quarterly and aims to publish articles of interest to both physicians and scientists. YJBM is and has been an internationally distributed journal with a long history of landmark articles. Our contributors feature a notable list of philosophers, statesmen, scientists, and physicians, including Ernst Cassirer, Harvey Cushing, Rene Dubos, Edward Kennedy, Donald Seldin, and Jack Strominger. Our Editorial Board consists of students and faculty members from Yale School of Medicine and Yale University Graduate School of Arts & Sciences. All manuscripts submitted to YJBM are first evaluated on the basis of scientific quality, originality, appropriateness, contribution to the field, and style. Suitable manuscripts are then subject to rigorous, fair, and rapid peer review.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
