Till D Lerch, Young-Jo Kim, Ata Kiapour, Adam Boschung, Simon D Steppacher, Moritz Tannast, Klaus A Siebenrock, Eduardo N Novais
{"title":"严重SCFE患者原位钉扎后的髋关节撞击导致3D-CT上屈曲减少和强迫外旋。","authors":"Till D Lerch, Young-Jo Kim, Ata Kiapour, Adam Boschung, Simon D Steppacher, Moritz Tannast, Klaus A Siebenrock, Eduardo N Novais","doi":"10.1177/18632521231192462","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>In situ pinning is an accepted treatment for stable slipped capital femoral epiphysis. However, residual deformity of severe slipped capital femoral epiphysis can cause femoroacetabular impingement and forced external rotation.</p><p><strong>Purpose/questions: </strong>The aim of this study was to evaluate the (1) hip external rotation and internal rotation in flexion, (2) hip impingement location, and (3) impingement frequency in early flexion in severe slipped capital femoral epiphysis patients after in situ pinning using three-dimensional computed tomography.</p><p><strong>Patients and methods: </strong>A retrospective Institutional Review Board-approved study evaluating 22 patients (26 hips) with severe slipped capital femoral epiphysis (slip angle > 60°) using postoperative three-dimensional computed tomography after in situ pinning was performed. Mean age at slipped capital femoral epiphysis diagnosis was 13 ± 2 years (58% male, four patients bilateral, 23% unstable, 85% chronic). Patients were compared to contralateral asymptomatic hips (15 hips) with unilateral slipped capital femoral epiphysis (control group). Pelvic three-dimensional computed tomography after in situ pinning was used to generate three-dimensional models. Specific software was used to determine range of motion and impingement location (equidistant method). And 22 hips (85%) underwent subsequent surgery.</p><p><strong>Results: </strong>(1) Severe slipped capital femoral epiphysis patients had significantly (p < 0.001) decreased hip flexion (43 ± 40°) and internal rotation in 90° of flexion (-16 ± 21°, IRF-90°) compared to control group (122 ± 9° and 36 ± 11°). (2) Femoral impingement in maximal flexion was located anterior to anterior-superior (27% on 3 o'clock and 27% on 1 o'clock) of severe slipped capital femoral epiphysis patients and located anterior to anterior-inferior (38% on 3 o'clock and 35% on 4 o'clock) in IRF-90°. (3) However, 21 hips (81%) had flexion < 90° and 22 hips (85%) had < 10° of IRF-90° due to hip impingement and 21 hips (81%) had forced external rotation in 90° of flexion (< 0° of IRF-90°).</p><p><strong>Conclusion: </strong>After in situ pinning, patient-specific three-dimensional models showed restricted flexion and IRF-90° and forced external rotation in 90° of flexion due to early hip impingement and residual deformity in most of the severe slipped capital femoral epiphysis patients. This could help to plan subsequent hip preservation surgery, such as hip arthroscopy or femoral (derotation) osteotomy.</p>","PeriodicalId":56060,"journal":{"name":"Journal of Childrens Orthopaedics","volume":"17 5","pages":"411-419"},"PeriodicalIF":1.6000,"publicationDate":"2023-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9b/d6/10.1177_18632521231192462.PMC10549698.pdf","citationCount":"0","resultStr":"{\"title\":\"Hip Impingement of severe SCFE patients after in situ pinning causes decreased flexion and forced external rotation in flexion on 3D-CT.\",\"authors\":\"Till D Lerch, Young-Jo Kim, Ata Kiapour, Adam Boschung, Simon D Steppacher, Moritz Tannast, Klaus A Siebenrock, Eduardo N Novais\",\"doi\":\"10.1177/18632521231192462\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>In situ pinning is an accepted treatment for stable slipped capital femoral epiphysis. However, residual deformity of severe slipped capital femoral epiphysis can cause femoroacetabular impingement and forced external rotation.</p><p><strong>Purpose/questions: </strong>The aim of this study was to evaluate the (1) hip external rotation and internal rotation in flexion, (2) hip impingement location, and (3) impingement frequency in early flexion in severe slipped capital femoral epiphysis patients after in situ pinning using three-dimensional computed tomography.</p><p><strong>Patients and methods: </strong>A retrospective Institutional Review Board-approved study evaluating 22 patients (26 hips) with severe slipped capital femoral epiphysis (slip angle > 60°) using postoperative three-dimensional computed tomography after in situ pinning was performed. Mean age at slipped capital femoral epiphysis diagnosis was 13 ± 2 years (58% male, four patients bilateral, 23% unstable, 85% chronic). Patients were compared to contralateral asymptomatic hips (15 hips) with unilateral slipped capital femoral epiphysis (control group). Pelvic three-dimensional computed tomography after in situ pinning was used to generate three-dimensional models. Specific software was used to determine range of motion and impingement location (equidistant method). And 22 hips (85%) underwent subsequent surgery.</p><p><strong>Results: </strong>(1) Severe slipped capital femoral epiphysis patients had significantly (p < 0.001) decreased hip flexion (43 ± 40°) and internal rotation in 90° of flexion (-16 ± 21°, IRF-90°) compared to control group (122 ± 9° and 36 ± 11°). (2) Femoral impingement in maximal flexion was located anterior to anterior-superior (27% on 3 o'clock and 27% on 1 o'clock) of severe slipped capital femoral epiphysis patients and located anterior to anterior-inferior (38% on 3 o'clock and 35% on 4 o'clock) in IRF-90°. (3) However, 21 hips (81%) had flexion < 90° and 22 hips (85%) had < 10° of IRF-90° due to hip impingement and 21 hips (81%) had forced external rotation in 90° of flexion (< 0° of IRF-90°).</p><p><strong>Conclusion: </strong>After in situ pinning, patient-specific three-dimensional models showed restricted flexion and IRF-90° and forced external rotation in 90° of flexion due to early hip impingement and residual deformity in most of the severe slipped capital femoral epiphysis patients. This could help to plan subsequent hip preservation surgery, such as hip arthroscopy or femoral (derotation) osteotomy.</p>\",\"PeriodicalId\":56060,\"journal\":{\"name\":\"Journal of Childrens Orthopaedics\",\"volume\":\"17 5\",\"pages\":\"411-419\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2023-08-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9b/d6/10.1177_18632521231192462.PMC10549698.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Childrens Orthopaedics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/18632521231192462\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Childrens Orthopaedics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/18632521231192462","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Hip Impingement of severe SCFE patients after in situ pinning causes decreased flexion and forced external rotation in flexion on 3D-CT.
Introduction: In situ pinning is an accepted treatment for stable slipped capital femoral epiphysis. However, residual deformity of severe slipped capital femoral epiphysis can cause femoroacetabular impingement and forced external rotation.
Purpose/questions: The aim of this study was to evaluate the (1) hip external rotation and internal rotation in flexion, (2) hip impingement location, and (3) impingement frequency in early flexion in severe slipped capital femoral epiphysis patients after in situ pinning using three-dimensional computed tomography.
Patients and methods: A retrospective Institutional Review Board-approved study evaluating 22 patients (26 hips) with severe slipped capital femoral epiphysis (slip angle > 60°) using postoperative three-dimensional computed tomography after in situ pinning was performed. Mean age at slipped capital femoral epiphysis diagnosis was 13 ± 2 years (58% male, four patients bilateral, 23% unstable, 85% chronic). Patients were compared to contralateral asymptomatic hips (15 hips) with unilateral slipped capital femoral epiphysis (control group). Pelvic three-dimensional computed tomography after in situ pinning was used to generate three-dimensional models. Specific software was used to determine range of motion and impingement location (equidistant method). And 22 hips (85%) underwent subsequent surgery.
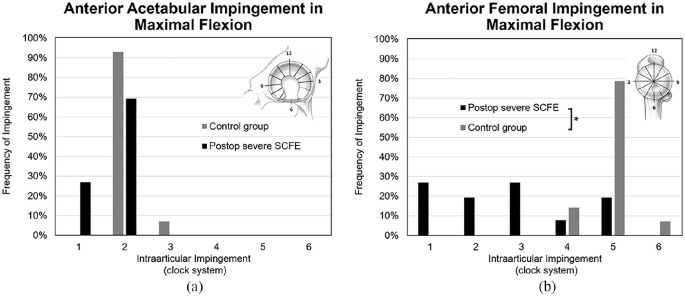
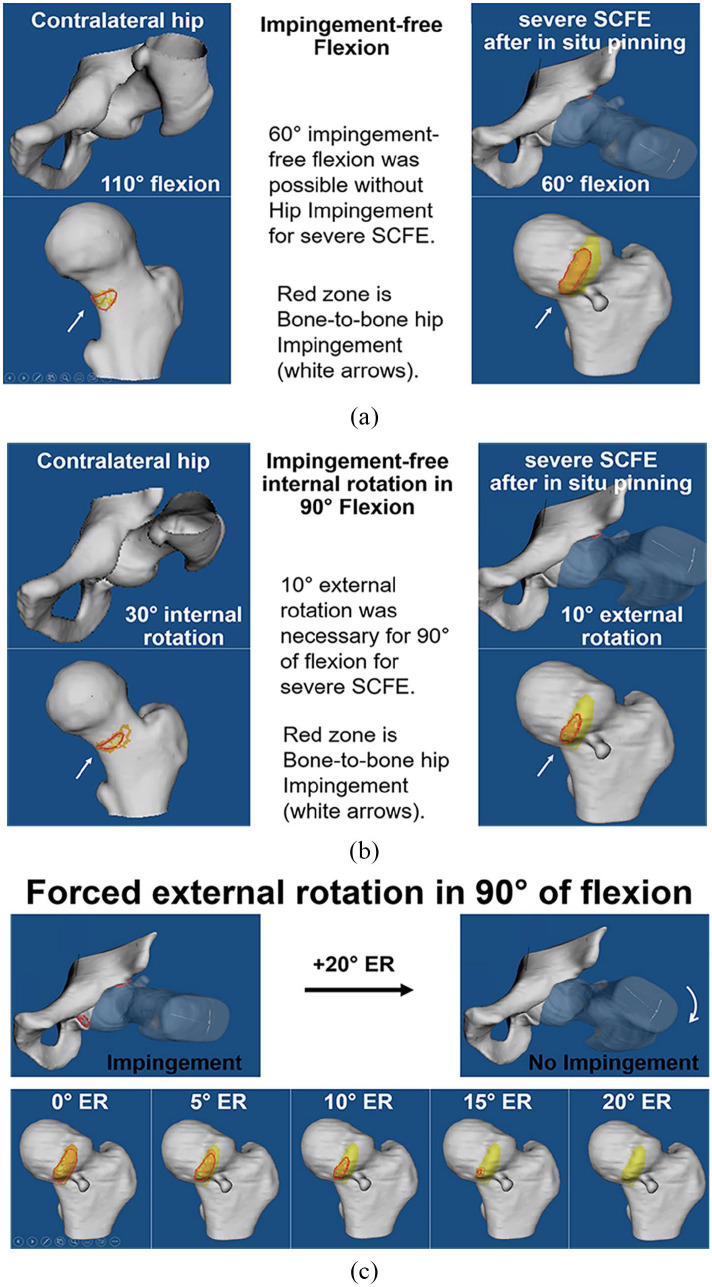
Results: (1) Severe slipped capital femoral epiphysis patients had significantly (p < 0.001) decreased hip flexion (43 ± 40°) and internal rotation in 90° of flexion (-16 ± 21°, IRF-90°) compared to control group (122 ± 9° and 36 ± 11°). (2) Femoral impingement in maximal flexion was located anterior to anterior-superior (27% on 3 o'clock and 27% on 1 o'clock) of severe slipped capital femoral epiphysis patients and located anterior to anterior-inferior (38% on 3 o'clock and 35% on 4 o'clock) in IRF-90°. (3) However, 21 hips (81%) had flexion < 90° and 22 hips (85%) had < 10° of IRF-90° due to hip impingement and 21 hips (81%) had forced external rotation in 90° of flexion (< 0° of IRF-90°).
Conclusion: After in situ pinning, patient-specific three-dimensional models showed restricted flexion and IRF-90° and forced external rotation in 90° of flexion due to early hip impingement and residual deformity in most of the severe slipped capital femoral epiphysis patients. This could help to plan subsequent hip preservation surgery, such as hip arthroscopy or femoral (derotation) osteotomy.
期刊介绍:
Aims & Scope
The Journal of Children’s Orthopaedics is the official journal of the European Paediatric Orthopaedic Society (EPOS) and is published by The British Editorial Society of Bone & Joint Surgery.
It provides a forum for the advancement of the knowledge and education in paediatric orthopaedics and traumatology across geographical borders. It advocates an increased worldwide involvement in preventing and treating musculoskeletal diseases in children and adolescents.
The journal publishes high quality, peer-reviewed articles that focus on clinical practice, diagnosis and treatment of disorders unique to paediatric orthopaedics, as well as on basic and applied research. It aims to help physicians stay abreast of the latest and ever-changing developments in the field of paediatric orthopaedics and traumatology.
The journal welcomes original contributions submitted exclusively for review to the journal. This continuously published online journal is fully open access and will publish one print issue each year to coincide with the EPOS Annual Congress, featuring the meeting’s abstracts.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
