Amir Haddad, Nili Stein, Idit Lavi, Lisa Shynkar, Irina Bergman, Ilan Feldhamer, Arnon Dov Cohen, Walid Saliba, Devy Zisman
{"title":"阿普利司特在银屑病关节炎患者中的治疗持续性。","authors":"Amir Haddad, Nili Stein, Idit Lavi, Lisa Shynkar, Irina Bergman, Ilan Feldhamer, Arnon Dov Cohen, Walid Saliba, Devy Zisman","doi":"10.2147/BTT.S425693","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Persistence in drug therapy reflects treatment effectiveness and tolerability. We aim to estimate the persistence of apremilast prescribed to patients with psoriatic arthritis (PsA) and to identify characteristics associated with treatment discontinuation in a real-world setting.</p><p><strong>Methods: </strong>Patients with PsA treated with apremilast from January 2016 were identified from a large health database and followed until medication stop date (using 3-months grace period), death or the end of observation period (June 2021). Demographic data, Charlson comorbidity index and concomitant and previous use of conventional and biologic DMARDs were extracted. The reasons for drug discontinuation were manually retrieved from patient charts. Time to discontinuation was estimated using survival analysis using Kaplan-Meier functions.</p><p><strong>Results: </strong>Overall, 568 PsA patients treated with apremilast were identified. The mean age was 55.3±14.0 years, of whom 332 (58.5%) were females, 38.4% were obese (BMI>30), 75.2% had a Charlson comorbidity index>1, 24.1% were on concomitant treatment with methotrexate and 72.4% were biologic naïve. The median persistent period was 6.1,95% CI (5.2-6.9) months in which only 16.9% remained persistent on apremilast. No difference was found with regard to age, sex, socioeconomic status, ethnicity and obesity between patients who were persistent compared to patients who discontinued apremilast. Concomitant treatment with methotrexate and prior history of biologic therapy did not affect drug persistency (log rank P=0.957 and 0.082, respectively). Causes for treatment discontinuation were due to lack of skin efficacy in 19.4%, lack of joint efficacy in 33.3%, combined skin and joint inefficacy at 2.3% and due to side effects in 24.1%.</p><p><strong>Conclusion: </strong>In this large observational retrospective cohort of patients treated with apremilast, a relatively low drug persistence was observed with 6-month and 1-year survival rates of 50.3% and 31.3%, respectively. Treatment discontinuation was mainly due to joint inefficacy, advocating for more studies for proper patient selection to assure treatment effectiveness and persistency.</p>","PeriodicalId":9025,"journal":{"name":"Biologics : Targets & Therapy","volume":"17 ","pages":"129-136"},"PeriodicalIF":5.3000,"publicationDate":"2023-10-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d9/bd/btt-17-129.PMC10560465.pdf","citationCount":"0","resultStr":"{\"title\":\"Treatment Persistence of Apremilast Among Patients with Psoriatic Arthritis.\",\"authors\":\"Amir Haddad, Nili Stein, Idit Lavi, Lisa Shynkar, Irina Bergman, Ilan Feldhamer, Arnon Dov Cohen, Walid Saliba, Devy Zisman\",\"doi\":\"10.2147/BTT.S425693\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Persistence in drug therapy reflects treatment effectiveness and tolerability. We aim to estimate the persistence of apremilast prescribed to patients with psoriatic arthritis (PsA) and to identify characteristics associated with treatment discontinuation in a real-world setting.</p><p><strong>Methods: </strong>Patients with PsA treated with apremilast from January 2016 were identified from a large health database and followed until medication stop date (using 3-months grace period), death or the end of observation period (June 2021). Demographic data, Charlson comorbidity index and concomitant and previous use of conventional and biologic DMARDs were extracted. The reasons for drug discontinuation were manually retrieved from patient charts. Time to discontinuation was estimated using survival analysis using Kaplan-Meier functions.</p><p><strong>Results: </strong>Overall, 568 PsA patients treated with apremilast were identified. The mean age was 55.3±14.0 years, of whom 332 (58.5%) were females, 38.4% were obese (BMI>30), 75.2% had a Charlson comorbidity index>1, 24.1% were on concomitant treatment with methotrexate and 72.4% were biologic naïve. The median persistent period was 6.1,95% CI (5.2-6.9) months in which only 16.9% remained persistent on apremilast. No difference was found with regard to age, sex, socioeconomic status, ethnicity and obesity between patients who were persistent compared to patients who discontinued apremilast. Concomitant treatment with methotrexate and prior history of biologic therapy did not affect drug persistency (log rank P=0.957 and 0.082, respectively). Causes for treatment discontinuation were due to lack of skin efficacy in 19.4%, lack of joint efficacy in 33.3%, combined skin and joint inefficacy at 2.3% and due to side effects in 24.1%.</p><p><strong>Conclusion: </strong>In this large observational retrospective cohort of patients treated with apremilast, a relatively low drug persistence was observed with 6-month and 1-year survival rates of 50.3% and 31.3%, respectively. Treatment discontinuation was mainly due to joint inefficacy, advocating for more studies for proper patient selection to assure treatment effectiveness and persistency.</p>\",\"PeriodicalId\":9025,\"journal\":{\"name\":\"Biologics : Targets & Therapy\",\"volume\":\"17 \",\"pages\":\"129-136\"},\"PeriodicalIF\":5.3000,\"publicationDate\":\"2023-10-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d9/bd/btt-17-129.PMC10560465.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Biologics : Targets & Therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/BTT.S425693\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biologics : Targets & Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/BTT.S425693","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
Treatment Persistence of Apremilast Among Patients with Psoriatic Arthritis.
Introduction: Persistence in drug therapy reflects treatment effectiveness and tolerability. We aim to estimate the persistence of apremilast prescribed to patients with psoriatic arthritis (PsA) and to identify characteristics associated with treatment discontinuation in a real-world setting.
Methods: Patients with PsA treated with apremilast from January 2016 were identified from a large health database and followed until medication stop date (using 3-months grace period), death or the end of observation period (June 2021). Demographic data, Charlson comorbidity index and concomitant and previous use of conventional and biologic DMARDs were extracted. The reasons for drug discontinuation were manually retrieved from patient charts. Time to discontinuation was estimated using survival analysis using Kaplan-Meier functions.
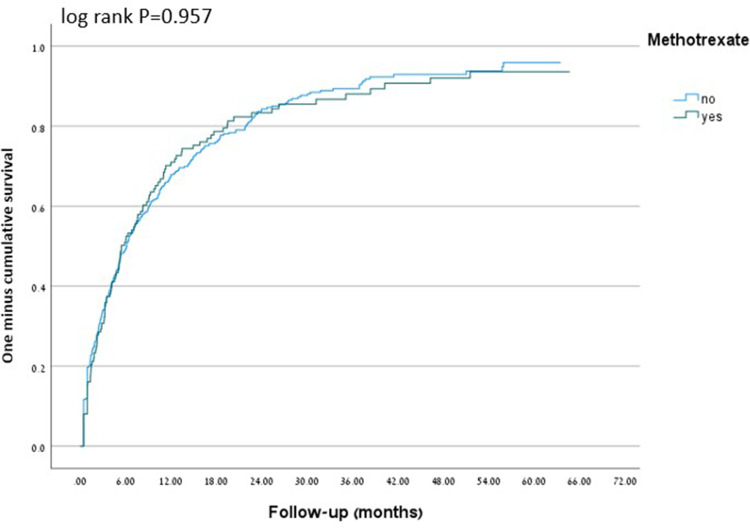
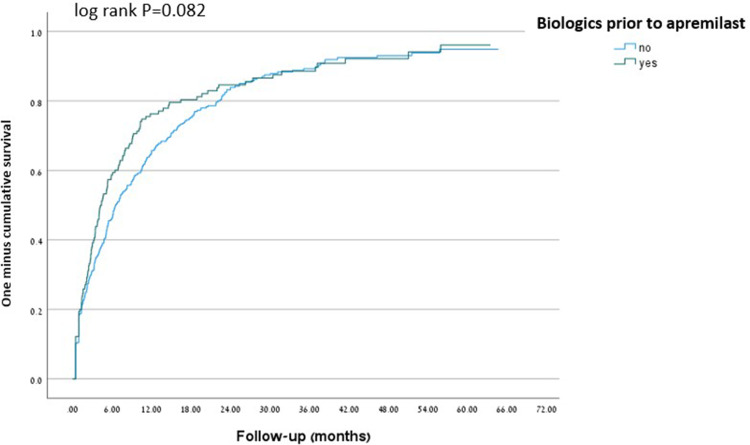
Results: Overall, 568 PsA patients treated with apremilast were identified. The mean age was 55.3±14.0 years, of whom 332 (58.5%) were females, 38.4% were obese (BMI>30), 75.2% had a Charlson comorbidity index>1, 24.1% were on concomitant treatment with methotrexate and 72.4% were biologic naïve. The median persistent period was 6.1,95% CI (5.2-6.9) months in which only 16.9% remained persistent on apremilast. No difference was found with regard to age, sex, socioeconomic status, ethnicity and obesity between patients who were persistent compared to patients who discontinued apremilast. Concomitant treatment with methotrexate and prior history of biologic therapy did not affect drug persistency (log rank P=0.957 and 0.082, respectively). Causes for treatment discontinuation were due to lack of skin efficacy in 19.4%, lack of joint efficacy in 33.3%, combined skin and joint inefficacy at 2.3% and due to side effects in 24.1%.
Conclusion: In this large observational retrospective cohort of patients treated with apremilast, a relatively low drug persistence was observed with 6-month and 1-year survival rates of 50.3% and 31.3%, respectively. Treatment discontinuation was mainly due to joint inefficacy, advocating for more studies for proper patient selection to assure treatment effectiveness and persistency.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
