Martin B. Thomsen, Jakob Nyvad, Kent L. Christensen, Mark Reinhard, Niels Henrik Buus
{"title":"24小时动态血压监测中的高与低测量频率——一项随机交叉研究。","authors":"Martin B. Thomsen, Jakob Nyvad, Kent L. Christensen, Mark Reinhard, Niels Henrik Buus","doi":"10.1038/s41371-023-00868-0","DOIUrl":null,"url":null,"abstract":"Ambulatory blood pressure monitoring (ABPM) may be stressful and associated with discomfort, possibly influenced by the number of cuff inflations. We compared a low frequency (LF-ABPM) regimen with one cuff inflation per hour, with a high frequency (HF-ABPM) regimen performed according to current guidelines using three cuff-inflations per hour during daytime and two cuff-inflations during night time. In a crossover study, patients underwent ABPMs with both frequencies, in a randomized order, within an interval of a few days. Patients reported pain (visual analogue scale from 0 to 10) and sleep disturbances after each ABPM. The primary endpoint was the difference in mean 24 h systolic BP (SBP) between HF-ABPM and LF-ABPM. A total of 171 patients were randomized, and data from 131 (age 58 ± 14 years, 47% females, 24% normotensive, 53% mildly hypertensive, and 22% moderately-severely hypertensive) completing both ABPMs were included in the analysis. Mean SBP was 137.5 mmHg (95% CI, 134.8;140.2) for HF-ABPM and 138.2 mmHg (95%CI, 135.2;141.1) for LF-ABPM. The 95% limits of agreement were −15.3 mmHg and +14.0 mmHg. Mean 24 h SBP difference between HF-ABPM and LF-ABPM was −0.7 mmHg (95%CI, −2.0;0.6). Coefficients of variation were similar for LF-ABPM and HF-ABPM. Pain scores (median with interquartile range), for HF-ABPM and LF-ABPM were 1.5 (0.6;3.0) and 1.3 (0.6;2.9) during daytime, and 1.3 (0.4:3.4) and 0.9 (0.4;2.0) during nighttime (P < 0.05 for both differences). We conclude that LF-ABPM and HF-ABPM values are in good agreement without any clinically relevant differences in BP. Furthermore, LF-ABPM causes a relatively modest reduction in procedure-related pain.","PeriodicalId":16070,"journal":{"name":"Journal of Human Hypertension","volume":"38 2","pages":"146-154"},"PeriodicalIF":3.4000,"publicationDate":"2023-10-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.nature.com/articles/s41371-023-00868-0.pdf","citationCount":"0","resultStr":"{\"title\":\"High versus low measurement frequency during 24-h ambulatory blood pressure monitoring - a randomized crossover study\",\"authors\":\"Martin B. Thomsen, Jakob Nyvad, Kent L. Christensen, Mark Reinhard, Niels Henrik Buus\",\"doi\":\"10.1038/s41371-023-00868-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Ambulatory blood pressure monitoring (ABPM) may be stressful and associated with discomfort, possibly influenced by the number of cuff inflations. We compared a low frequency (LF-ABPM) regimen with one cuff inflation per hour, with a high frequency (HF-ABPM) regimen performed according to current guidelines using three cuff-inflations per hour during daytime and two cuff-inflations during night time. In a crossover study, patients underwent ABPMs with both frequencies, in a randomized order, within an interval of a few days. Patients reported pain (visual analogue scale from 0 to 10) and sleep disturbances after each ABPM. The primary endpoint was the difference in mean 24 h systolic BP (SBP) between HF-ABPM and LF-ABPM. A total of 171 patients were randomized, and data from 131 (age 58 ± 14 years, 47% females, 24% normotensive, 53% mildly hypertensive, and 22% moderately-severely hypertensive) completing both ABPMs were included in the analysis. Mean SBP was 137.5 mmHg (95% CI, 134.8;140.2) for HF-ABPM and 138.2 mmHg (95%CI, 135.2;141.1) for LF-ABPM. The 95% limits of agreement were −15.3 mmHg and +14.0 mmHg. Mean 24 h SBP difference between HF-ABPM and LF-ABPM was −0.7 mmHg (95%CI, −2.0;0.6). Coefficients of variation were similar for LF-ABPM and HF-ABPM. Pain scores (median with interquartile range), for HF-ABPM and LF-ABPM were 1.5 (0.6;3.0) and 1.3 (0.6;2.9) during daytime, and 1.3 (0.4:3.4) and 0.9 (0.4;2.0) during nighttime (P < 0.05 for both differences). We conclude that LF-ABPM and HF-ABPM values are in good agreement without any clinically relevant differences in BP. Furthermore, LF-ABPM causes a relatively modest reduction in procedure-related pain.\",\"PeriodicalId\":16070,\"journal\":{\"name\":\"Journal of Human Hypertension\",\"volume\":\"38 2\",\"pages\":\"146-154\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2023-10-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.nature.com/articles/s41371-023-00868-0.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Human Hypertension\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.nature.com/articles/s41371-023-00868-0\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Human Hypertension","FirstCategoryId":"3","ListUrlMain":"https://www.nature.com/articles/s41371-023-00868-0","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
摘要
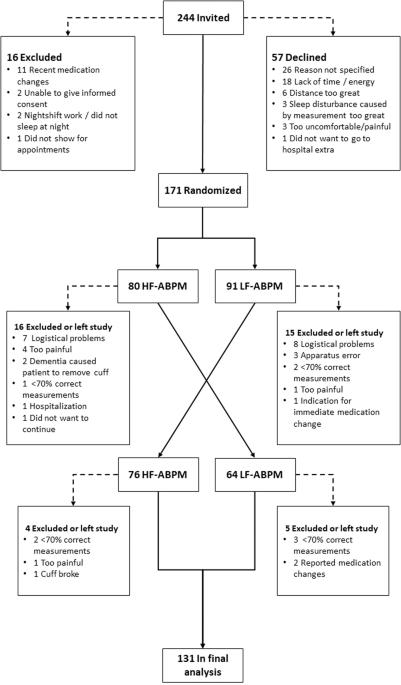
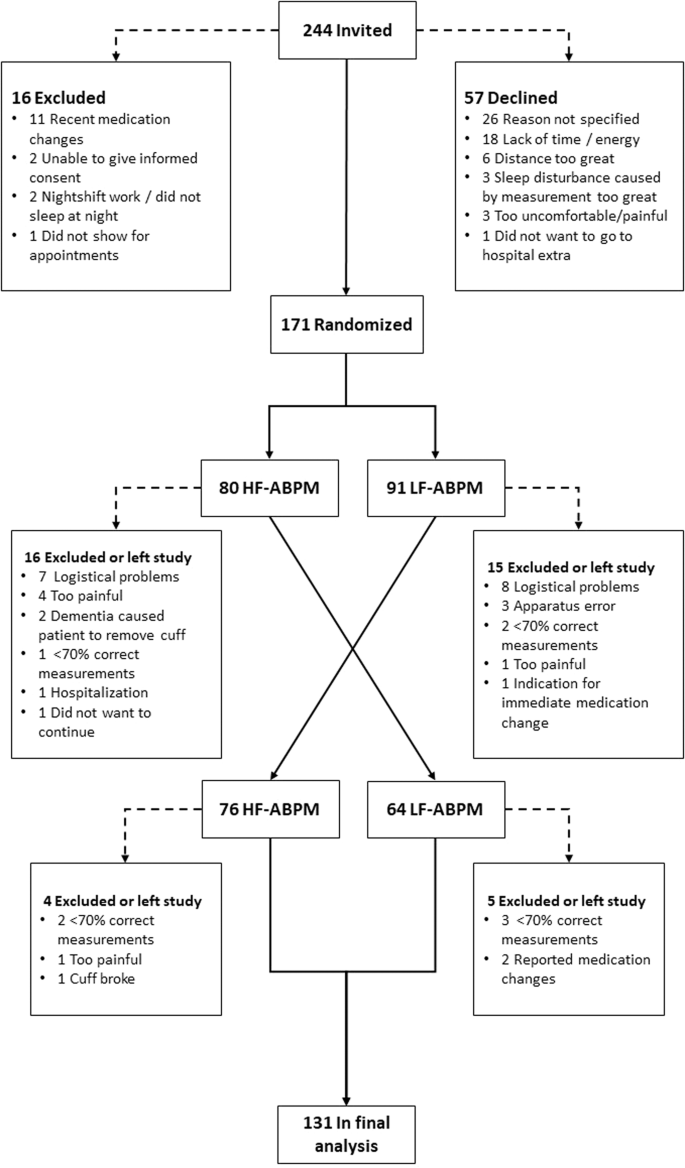
动态血压监测(ABPM)可能有压力,并与不适有关,可能受到袖带充气次数的影响。我们将低频(LF-ABPM)方案与高频(HF-ABPM)方法进行了比较,前者为每小时一次袖带充气,后者根据当前指南进行,白天为每小时三次,夜间为每小时两次。在一项交叉研究中,患者在几天内以随机顺序接受了两种频率的ABPM。患者在每次ABPM后报告疼痛(视觉模拟量表从0到10)和睡眠障碍。主要终点是平均24 h HF-ABPM和LF-ABPM之间的收缩压(SBP)。共有171名患者被随机分组,数据来自131名(年龄58岁) ± 14岁,47%的女性,24%的血压正常,53%的轻度高血压,22%的中度重度高血压)完成两项ABPM。平均收缩压为137.5 HF-ABPM和138.2的mmHg(95%CI,134.8;140.2) LF-ABPM为mmHg(95%CI,135.2;141.1)。95%的协议限制为-15.3 mmHg和+14.0 mmHg。平均24 h HF-ABPM和LF-ABPM之间的SBP差异为-0.7 mmHg(95%CI,-2.0;0.6)。LF-ABPM和HF-ABPM的变异系数相似。HF-ABPM和LF-ABPM的疼痛评分(四分位间距中位数)白天分别为1.5(0.6;3.0)和1.3(0.6;2.9),夜间分别为1.3(0.4:3.4)和0.9(0.4;2.0)(P
High versus low measurement frequency during 24-h ambulatory blood pressure monitoring - a randomized crossover study
Ambulatory blood pressure monitoring (ABPM) may be stressful and associated with discomfort, possibly influenced by the number of cuff inflations. We compared a low frequency (LF-ABPM) regimen with one cuff inflation per hour, with a high frequency (HF-ABPM) regimen performed according to current guidelines using three cuff-inflations per hour during daytime and two cuff-inflations during night time. In a crossover study, patients underwent ABPMs with both frequencies, in a randomized order, within an interval of a few days. Patients reported pain (visual analogue scale from 0 to 10) and sleep disturbances after each ABPM. The primary endpoint was the difference in mean 24 h systolic BP (SBP) between HF-ABPM and LF-ABPM. A total of 171 patients were randomized, and data from 131 (age 58 ± 14 years, 47% females, 24% normotensive, 53% mildly hypertensive, and 22% moderately-severely hypertensive) completing both ABPMs were included in the analysis. Mean SBP was 137.5 mmHg (95% CI, 134.8;140.2) for HF-ABPM and 138.2 mmHg (95%CI, 135.2;141.1) for LF-ABPM. The 95% limits of agreement were −15.3 mmHg and +14.0 mmHg. Mean 24 h SBP difference between HF-ABPM and LF-ABPM was −0.7 mmHg (95%CI, −2.0;0.6). Coefficients of variation were similar for LF-ABPM and HF-ABPM. Pain scores (median with interquartile range), for HF-ABPM and LF-ABPM were 1.5 (0.6;3.0) and 1.3 (0.6;2.9) during daytime, and 1.3 (0.4:3.4) and 0.9 (0.4;2.0) during nighttime (P < 0.05 for both differences). We conclude that LF-ABPM and HF-ABPM values are in good agreement without any clinically relevant differences in BP. Furthermore, LF-ABPM causes a relatively modest reduction in procedure-related pain.
期刊介绍:
Journal of Human Hypertension is published monthly and is of interest to health care professionals who deal with hypertension (specialists, internists, primary care physicians) and public health workers. We believe that our patients benefit from robust scientific data that are based on well conducted clinical trials. We also believe that basic sciences are the foundations on which we build our knowledge of clinical conditions and their management. Towards this end, although we are primarily a clinical based journal, we also welcome suitable basic sciences studies that promote our understanding of human hypertension.
The journal aims to perform the dual role of increasing knowledge in the field of high blood pressure as well as improving the standard of care of patients. The editors will consider for publication all suitable papers dealing directly or indirectly with clinical aspects of hypertension, including but not limited to epidemiology, pathophysiology, therapeutics and basic sciences involving human subjects or tissues. We also consider papers from all specialties such as ophthalmology, cardiology, nephrology, obstetrics and stroke medicine that deal with the various aspects of hypertension and its complications.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
