Muhammad Ali Tariq, Minhail Khalid Malik, Qazi Shurjeel Uddin, Zahabia Altaf, Mariam Zafar
{"title":"既往心脏手术患者二尖瓣手术的微创手术与传统重做立体术:系统综述和荟萃分析。","authors":"Muhammad Ali Tariq, Minhail Khalid Malik, Qazi Shurjeel Uddin, Zahabia Altaf, Mariam Zafar","doi":"10.5090/jcs.23.038","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The heightened morbidity and mortality associated with repeat cardiac surgery are well documented. Redo median sternotomy (MS) and minimally invasive valve surgery are options for patients with prior cardiac surgery who require mitral valve surgery (MVS). We conducted a systematic review and meta-analysis comparing the outcomes of redo MS and minimally invasive MVS (MIMVS) in this population.</p><p><strong>Methods: </strong>We searched PubMed, EMBASE, and Scopus for studies comparing outcomes of redo MS and MIMVS for MVS. To calculate risk ratios (RRs) for binary outcomes and weighted mean differences (MDs) for continuous data, we employed a random-effects model.</p><p><strong>Results: </strong>We included 12 retrospective observational studies, comprising 4157 participants (675 for MIMVS; 3482 for redo MS). Reductions in mortality (RR, 0.54; 95% confidence interval [CI], 0.37-0.80), length of hospital stay (MD, -4.23; 95% CI, -5.77 to -2.68), length of intensive care unit (ICU) stay (MD, -2.02; 95% CI, -3.17 to -0.88), and new-onset acute kidney injury (AKI) risk (odds ratio, 0.34; 95% CI, 0.19 to 0.61) were statistically significant and favored MIMVS (p<0.05). No significant differences were observed in aortic cross-clamp time, cardiopulmonary bypass time, or risk of perioperative stroke, new-onset atrial fibrillation, surgical site infection, or reoperation for bleeding (p>0.05).</p><p><strong>Conclusion: </strong>The current literature, which primarily consists of retrospective comparisons, underscores certain benefits of MIMVS over redo MS. These include decreased mortality, shorter hospital and ICU stays, and reduced AKI risk. Given the lack of high-quality evidence, prospective randomized control trials with adequate power are necessary to investigate long-term outcomes.</p>","PeriodicalId":34499,"journal":{"name":"Journal of Chest Surgery","volume":" ","pages":"374-386"},"PeriodicalIF":1.0000,"publicationDate":"2023-11-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10625962/pdf/","citationCount":"0","resultStr":"{\"title\":\"Minimally Invasive Procedure versus Conventional Redo Sternotomy for Mitral Valve Surgery in Patients with Previous Cardiac Surgery: A Systematic Review and Meta-Analysis.\",\"authors\":\"Muhammad Ali Tariq, Minhail Khalid Malik, Qazi Shurjeel Uddin, Zahabia Altaf, Mariam Zafar\",\"doi\":\"10.5090/jcs.23.038\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The heightened morbidity and mortality associated with repeat cardiac surgery are well documented. Redo median sternotomy (MS) and minimally invasive valve surgery are options for patients with prior cardiac surgery who require mitral valve surgery (MVS). We conducted a systematic review and meta-analysis comparing the outcomes of redo MS and minimally invasive MVS (MIMVS) in this population.</p><p><strong>Methods: </strong>We searched PubMed, EMBASE, and Scopus for studies comparing outcomes of redo MS and MIMVS for MVS. To calculate risk ratios (RRs) for binary outcomes and weighted mean differences (MDs) for continuous data, we employed a random-effects model.</p><p><strong>Results: </strong>We included 12 retrospective observational studies, comprising 4157 participants (675 for MIMVS; 3482 for redo MS). Reductions in mortality (RR, 0.54; 95% confidence interval [CI], 0.37-0.80), length of hospital stay (MD, -4.23; 95% CI, -5.77 to -2.68), length of intensive care unit (ICU) stay (MD, -2.02; 95% CI, -3.17 to -0.88), and new-onset acute kidney injury (AKI) risk (odds ratio, 0.34; 95% CI, 0.19 to 0.61) were statistically significant and favored MIMVS (p<0.05). No significant differences were observed in aortic cross-clamp time, cardiopulmonary bypass time, or risk of perioperative stroke, new-onset atrial fibrillation, surgical site infection, or reoperation for bleeding (p>0.05).</p><p><strong>Conclusion: </strong>The current literature, which primarily consists of retrospective comparisons, underscores certain benefits of MIMVS over redo MS. These include decreased mortality, shorter hospital and ICU stays, and reduced AKI risk. Given the lack of high-quality evidence, prospective randomized control trials with adequate power are necessary to investigate long-term outcomes.</p>\",\"PeriodicalId\":34499,\"journal\":{\"name\":\"Journal of Chest Surgery\",\"volume\":\" \",\"pages\":\"374-386\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2023-11-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10625962/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Chest Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5090/jcs.23.038\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/10/11 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Chest Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5090/jcs.23.038","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/11 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
Minimally Invasive Procedure versus Conventional Redo Sternotomy for Mitral Valve Surgery in Patients with Previous Cardiac Surgery: A Systematic Review and Meta-Analysis.
Background: The heightened morbidity and mortality associated with repeat cardiac surgery are well documented. Redo median sternotomy (MS) and minimally invasive valve surgery are options for patients with prior cardiac surgery who require mitral valve surgery (MVS). We conducted a systematic review and meta-analysis comparing the outcomes of redo MS and minimally invasive MVS (MIMVS) in this population.
Methods: We searched PubMed, EMBASE, and Scopus for studies comparing outcomes of redo MS and MIMVS for MVS. To calculate risk ratios (RRs) for binary outcomes and weighted mean differences (MDs) for continuous data, we employed a random-effects model.
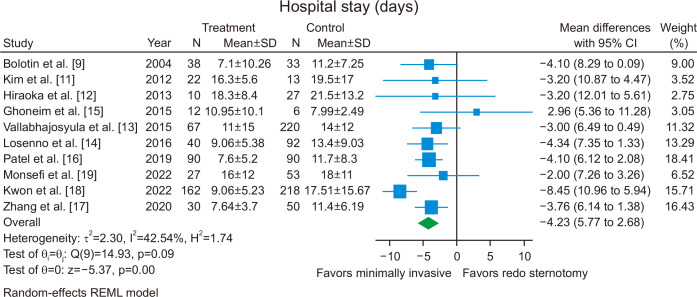
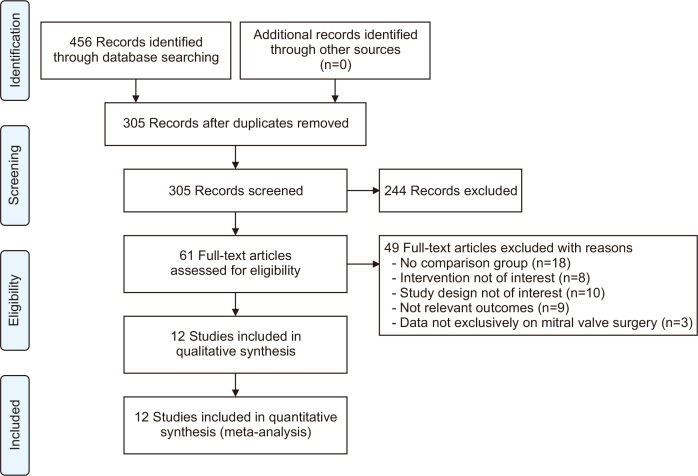
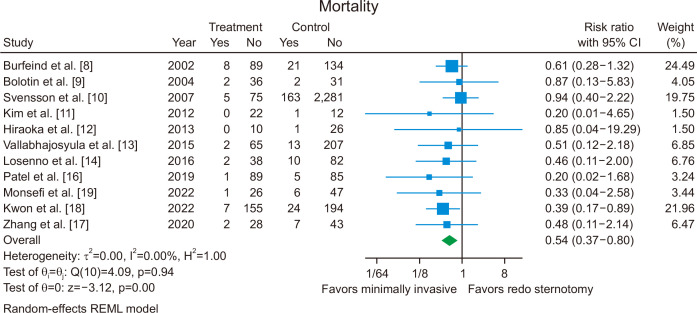
Results: We included 12 retrospective observational studies, comprising 4157 participants (675 for MIMVS; 3482 for redo MS). Reductions in mortality (RR, 0.54; 95% confidence interval [CI], 0.37-0.80), length of hospital stay (MD, -4.23; 95% CI, -5.77 to -2.68), length of intensive care unit (ICU) stay (MD, -2.02; 95% CI, -3.17 to -0.88), and new-onset acute kidney injury (AKI) risk (odds ratio, 0.34; 95% CI, 0.19 to 0.61) were statistically significant and favored MIMVS (p<0.05). No significant differences were observed in aortic cross-clamp time, cardiopulmonary bypass time, or risk of perioperative stroke, new-onset atrial fibrillation, surgical site infection, or reoperation for bleeding (p>0.05).
Conclusion: The current literature, which primarily consists of retrospective comparisons, underscores certain benefits of MIMVS over redo MS. These include decreased mortality, shorter hospital and ICU stays, and reduced AKI risk. Given the lack of high-quality evidence, prospective randomized control trials with adequate power are necessary to investigate long-term outcomes.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
