{"title":"心力衰竭住院患者左心室射血分数与治疗特点的关系——日本数据库分析。","authors":"Ichiro Umemura, Shunsuke Eguchi, Yohei Morita, Hironobu Mitani, Kazuma Iekushi, Takao Kato","doi":"10.1253/circrep.CR-23-0066","DOIUrl":null,"url":null,"abstract":"<p><p><b><i>Background:</i></b> Triple combination therapy with a renin-angiotensin system modulator, a β-blocker, and a mineralocorticoid receptor antagonist is currently recommended for patients with heart failure (HF) with reduced ejection fraction. However, there is limited evidence on the extent to which triple combination therapy is currently prescribed to patients at the time of discharge from hospital in Japan. <b><i>Methods and Results:</i></b> Japanese patients hospitalized for HF (n=3,582) were evaluated in subgroups defined by left ventricular ejection fraction (LVEF) using anonymized claims and electronic health record data. At discharge, triple combination therapy prescription rates were low (40.4%, 30.0%, 20.8%, 14.0%, and 12.5% for patients with LVEF <30%, 30-<40%, 40-<50%, 50-<60%, and ≥60%, respectively). Advanced age, lower levels of B-type natriuretic peptide, and renal impairment were all significantly associated with lower rates of triple combination therapy use in the overall population. There were no significant differences in rehospitalization rates between LVEF subgroups; however, triple combination therapy use was associated with a significantly reduced risk of rehospitalization for HF in patients with LVEF <30%, 30-<40%, and 40-<50%. <b><i>Conclusions:</i></b> The use of triple combination therapy was significantly associated with a lower risk of rehospitalization for HF within 1 year of discharge in patients with LVEF <30%, 30-<40%, and 40-<50%. However, patients were undertreated with triple combination therapy.</p>","PeriodicalId":94305,"journal":{"name":"Circulation reports","volume":"5 10","pages":"392-402"},"PeriodicalIF":1.1000,"publicationDate":"2023-09-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2f/09/circrep-5-392.PMC10561998.pdf","citationCount":"0","resultStr":"{\"title\":\"Relationship Between Left Ventricular Ejection Fraction and Treatment Characteristics in Hospitalized Patients With Heart Failure - A Japanese Database Analysis.\",\"authors\":\"Ichiro Umemura, Shunsuke Eguchi, Yohei Morita, Hironobu Mitani, Kazuma Iekushi, Takao Kato\",\"doi\":\"10.1253/circrep.CR-23-0066\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b><i>Background:</i></b> Triple combination therapy with a renin-angiotensin system modulator, a β-blocker, and a mineralocorticoid receptor antagonist is currently recommended for patients with heart failure (HF) with reduced ejection fraction. However, there is limited evidence on the extent to which triple combination therapy is currently prescribed to patients at the time of discharge from hospital in Japan. <b><i>Methods and Results:</i></b> Japanese patients hospitalized for HF (n=3,582) were evaluated in subgroups defined by left ventricular ejection fraction (LVEF) using anonymized claims and electronic health record data. At discharge, triple combination therapy prescription rates were low (40.4%, 30.0%, 20.8%, 14.0%, and 12.5% for patients with LVEF <30%, 30-<40%, 40-<50%, 50-<60%, and ≥60%, respectively). Advanced age, lower levels of B-type natriuretic peptide, and renal impairment were all significantly associated with lower rates of triple combination therapy use in the overall population. There were no significant differences in rehospitalization rates between LVEF subgroups; however, triple combination therapy use was associated with a significantly reduced risk of rehospitalization for HF in patients with LVEF <30%, 30-<40%, and 40-<50%. <b><i>Conclusions:</i></b> The use of triple combination therapy was significantly associated with a lower risk of rehospitalization for HF within 1 year of discharge in patients with LVEF <30%, 30-<40%, and 40-<50%. However, patients were undertreated with triple combination therapy.</p>\",\"PeriodicalId\":94305,\"journal\":{\"name\":\"Circulation reports\",\"volume\":\"5 10\",\"pages\":\"392-402\"},\"PeriodicalIF\":1.1000,\"publicationDate\":\"2023-09-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2f/09/circrep-5-392.PMC10561998.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Circulation reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1253/circrep.CR-23-0066\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/10/10 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1253/circrep.CR-23-0066","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/10 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Relationship Between Left Ventricular Ejection Fraction and Treatment Characteristics in Hospitalized Patients With Heart Failure - A Japanese Database Analysis.
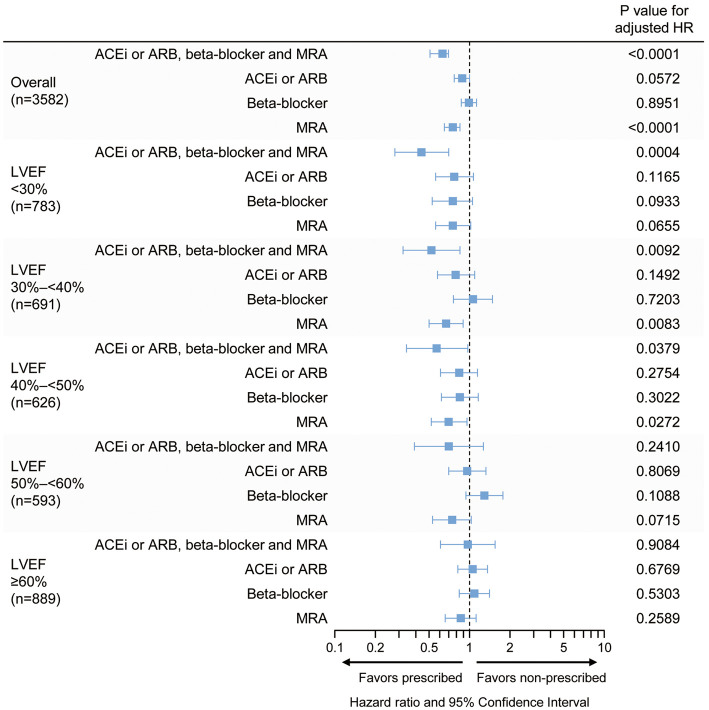
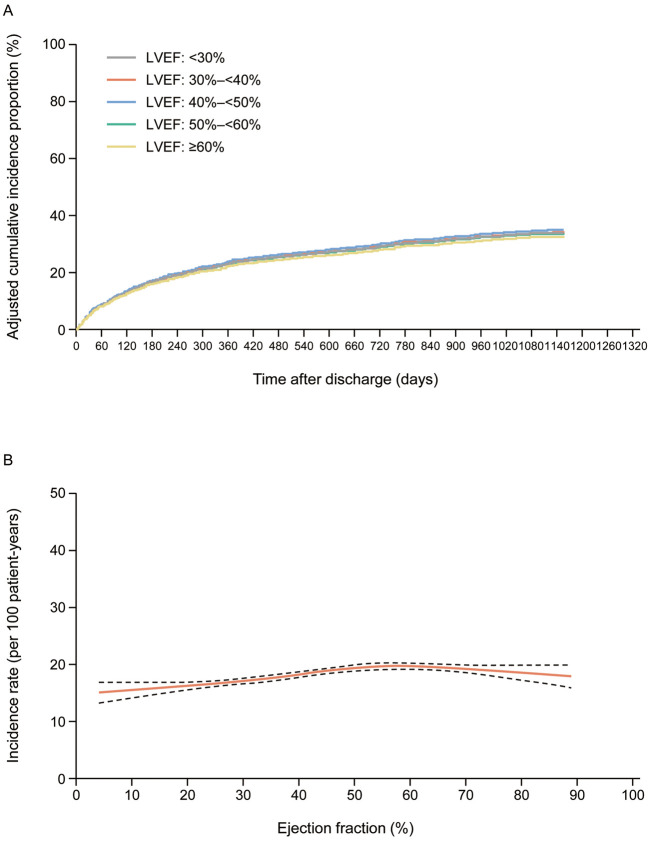
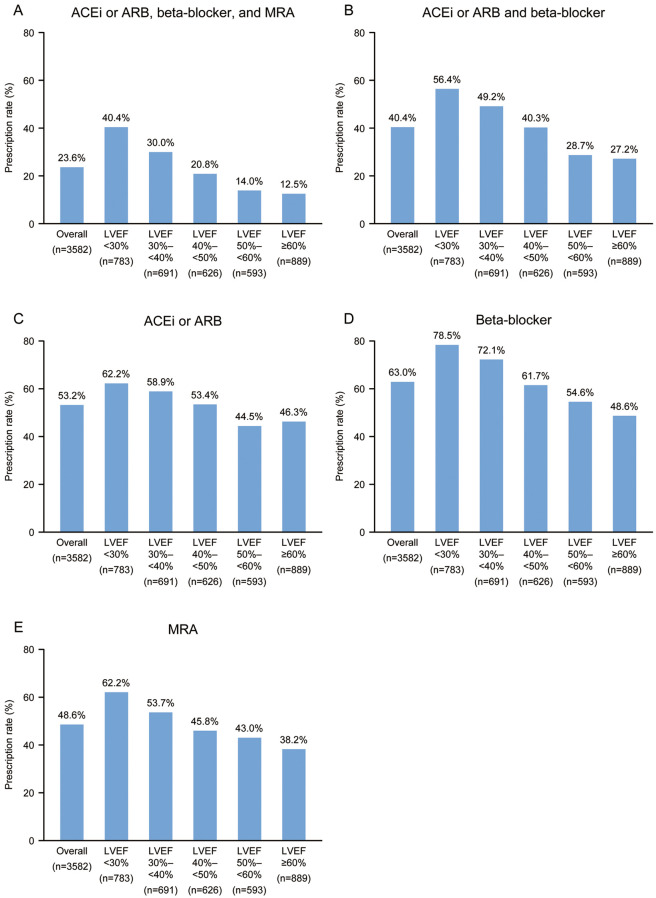
Background: Triple combination therapy with a renin-angiotensin system modulator, a β-blocker, and a mineralocorticoid receptor antagonist is currently recommended for patients with heart failure (HF) with reduced ejection fraction. However, there is limited evidence on the extent to which triple combination therapy is currently prescribed to patients at the time of discharge from hospital in Japan. Methods and Results: Japanese patients hospitalized for HF (n=3,582) were evaluated in subgroups defined by left ventricular ejection fraction (LVEF) using anonymized claims and electronic health record data. At discharge, triple combination therapy prescription rates were low (40.4%, 30.0%, 20.8%, 14.0%, and 12.5% for patients with LVEF <30%, 30-<40%, 40-<50%, 50-<60%, and ≥60%, respectively). Advanced age, lower levels of B-type natriuretic peptide, and renal impairment were all significantly associated with lower rates of triple combination therapy use in the overall population. There were no significant differences in rehospitalization rates between LVEF subgroups; however, triple combination therapy use was associated with a significantly reduced risk of rehospitalization for HF in patients with LVEF <30%, 30-<40%, and 40-<50%. Conclusions: The use of triple combination therapy was significantly associated with a lower risk of rehospitalization for HF within 1 year of discharge in patients with LVEF <30%, 30-<40%, and 40-<50%. However, patients were undertreated with triple combination therapy.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
