{"title":"椎间孔狭窄导致L5神经根病的无融合根治性减压。","authors":"Kohei Takahashi, Ajay Yadav, Takumi Tsubakino, Takeshi Hoshikawa, Tomowaki Nakagawa, Ko Hashimoto, Manabu Suzuki, Toshimi Aizawa, Yasuhisa Tanaka","doi":"10.21037/jss-23-62","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The highest incidence of lumbar foraminal stenosis (LFS) occurs in the L5-S1 segment and its anatomical features differ from those of other segments. Few previous reports have exhaustively assessed surgical outcomes after decompression surgery, limiting the materials to patients with LFS at the L5-S1 segment. We aimed to prospectively investigate instability and neurological improvement following our novel surgical technique for LFS at L5-S1, named \"radical decompression\" of the nerve root.</p><p><strong>Methods: </strong>Patients with foraminal stenosis at L5-S1 who underwent surgery using our technique were prospectively evaluated two years postoperatively. The Japanese Orthopaedic Association (JOA) score and the JOA Back Pain Evaluation Questionnaire (JOABPEQ) were evaluated preoperatively and two years postoperatively. The following radiological parameters at L5-S1 were measured: lateral translation, sagittal translation, the difference in sagittal translation (DST) between flexion and extension, disc wedging angle, lordotic angle, the difference in lordotic angle (DLA) between flexion and extension, and disc height. Pre- and postoperative data were compared using paired <i>t</i>-tests. In addition, the patients were classified into a disc group (Group D) and a non-disc group (Group ND) according to whether a discectomy was performed intraoperatively. Changes in each parameter before and after surgery were compared between the groups.</p><p><strong>Results: </strong>Twenty-eight patients were included in this analysis. The JOA scores improved in all patients. The mean preoperative and two-year postoperative JOA scores were 14.5±3.2 (range, 8-21) and 24.3±3.3 (range, 18-29), respectively (P<0.01). All JOABPEQ categories improved two years postoperatively (P<0.05). None of the patients underwent revision surgery. No significant changes were observed in any of the radiological parameters. No significant differences in the changes in each parameter before and after surgery were found between groups D and ND.</p><p><strong>Conclusions: </strong>Our surgical technique resulted in good neurological recovery and was associated with a low risk of postoperative segmental instability, regardless of additional discectomy.</p>","PeriodicalId":17131,"journal":{"name":"Journal of spine surgery","volume":"9 3","pages":"278-287"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e9/18/jss-09-03-278.PMC10570647.pdf","citationCount":"0","resultStr":"{\"title\":\"Radical decompression without fusion for L5 radiculopathy due to foraminal stenosis.\",\"authors\":\"Kohei Takahashi, Ajay Yadav, Takumi Tsubakino, Takeshi Hoshikawa, Tomowaki Nakagawa, Ko Hashimoto, Manabu Suzuki, Toshimi Aizawa, Yasuhisa Tanaka\",\"doi\":\"10.21037/jss-23-62\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The highest incidence of lumbar foraminal stenosis (LFS) occurs in the L5-S1 segment and its anatomical features differ from those of other segments. Few previous reports have exhaustively assessed surgical outcomes after decompression surgery, limiting the materials to patients with LFS at the L5-S1 segment. We aimed to prospectively investigate instability and neurological improvement following our novel surgical technique for LFS at L5-S1, named \\\"radical decompression\\\" of the nerve root.</p><p><strong>Methods: </strong>Patients with foraminal stenosis at L5-S1 who underwent surgery using our technique were prospectively evaluated two years postoperatively. The Japanese Orthopaedic Association (JOA) score and the JOA Back Pain Evaluation Questionnaire (JOABPEQ) were evaluated preoperatively and two years postoperatively. The following radiological parameters at L5-S1 were measured: lateral translation, sagittal translation, the difference in sagittal translation (DST) between flexion and extension, disc wedging angle, lordotic angle, the difference in lordotic angle (DLA) between flexion and extension, and disc height. Pre- and postoperative data were compared using paired <i>t</i>-tests. In addition, the patients were classified into a disc group (Group D) and a non-disc group (Group ND) according to whether a discectomy was performed intraoperatively. Changes in each parameter before and after surgery were compared between the groups.</p><p><strong>Results: </strong>Twenty-eight patients were included in this analysis. The JOA scores improved in all patients. The mean preoperative and two-year postoperative JOA scores were 14.5±3.2 (range, 8-21) and 24.3±3.3 (range, 18-29), respectively (P<0.01). All JOABPEQ categories improved two years postoperatively (P<0.05). None of the patients underwent revision surgery. No significant changes were observed in any of the radiological parameters. No significant differences in the changes in each parameter before and after surgery were found between groups D and ND.</p><p><strong>Conclusions: </strong>Our surgical technique resulted in good neurological recovery and was associated with a low risk of postoperative segmental instability, regardless of additional discectomy.</p>\",\"PeriodicalId\":17131,\"journal\":{\"name\":\"Journal of spine surgery\",\"volume\":\"9 3\",\"pages\":\"278-287\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-09-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e9/18/jss-09-03-278.PMC10570647.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of spine surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21037/jss-23-62\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/9/19 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of spine surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/jss-23-62","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/19 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
Radical decompression without fusion for L5 radiculopathy due to foraminal stenosis.
Background: The highest incidence of lumbar foraminal stenosis (LFS) occurs in the L5-S1 segment and its anatomical features differ from those of other segments. Few previous reports have exhaustively assessed surgical outcomes after decompression surgery, limiting the materials to patients with LFS at the L5-S1 segment. We aimed to prospectively investigate instability and neurological improvement following our novel surgical technique for LFS at L5-S1, named "radical decompression" of the nerve root.
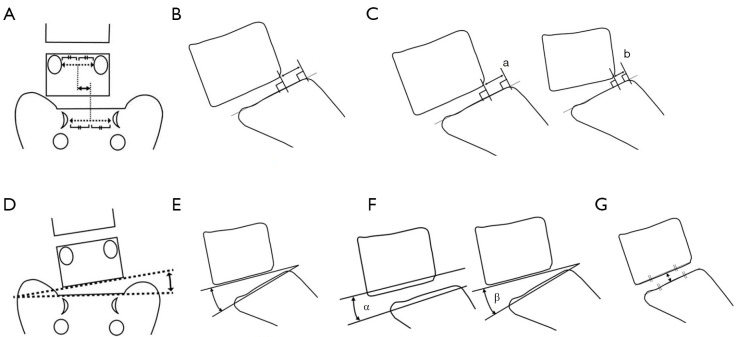
Methods: Patients with foraminal stenosis at L5-S1 who underwent surgery using our technique were prospectively evaluated two years postoperatively. The Japanese Orthopaedic Association (JOA) score and the JOA Back Pain Evaluation Questionnaire (JOABPEQ) were evaluated preoperatively and two years postoperatively. The following radiological parameters at L5-S1 were measured: lateral translation, sagittal translation, the difference in sagittal translation (DST) between flexion and extension, disc wedging angle, lordotic angle, the difference in lordotic angle (DLA) between flexion and extension, and disc height. Pre- and postoperative data were compared using paired t-tests. In addition, the patients were classified into a disc group (Group D) and a non-disc group (Group ND) according to whether a discectomy was performed intraoperatively. Changes in each parameter before and after surgery were compared between the groups.
Results: Twenty-eight patients were included in this analysis. The JOA scores improved in all patients. The mean preoperative and two-year postoperative JOA scores were 14.5±3.2 (range, 8-21) and 24.3±3.3 (range, 18-29), respectively (P<0.01). All JOABPEQ categories improved two years postoperatively (P<0.05). None of the patients underwent revision surgery. No significant changes were observed in any of the radiological parameters. No significant differences in the changes in each parameter before and after surgery were found between groups D and ND.
Conclusions: Our surgical technique resulted in good neurological recovery and was associated with a low risk of postoperative segmental instability, regardless of additional discectomy.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
