{"title":"分布式运动网络连通性的变化与脑肿瘤手术切除后的功能预后相关","authors":"Yukihiro Yamao, Nobukatsu Sawamoto, Takeharu Kunieda, Rika Inano, Sumiya Shibata, Takayuki Kikuchi, Yoshiki Arakawa, Kazumichi Yoshida, Riki Matsumoto, Akio Ikeda, Ryosuke Takahashi, Hidenao Fukuyama, Susumu Miyamoto","doi":"10.1227/neuprac.0000000000000028","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In patients with brain tumors around the motor cortices, deterioration of motor performance may be observed even if the integrity of the cortical output is maintained. Especially, resection of medial premotor area (PM) can cause postoperative deterioration called supplementary motor area syndrome.</p><p><strong>Objective: </strong>To clarify the neuronal mechanisms underlying postsurgical deterioration with a case-control study.</p><p><strong>Methods: </strong>Twelve patients with brain tumors underwent preoperative and postoperative sessions consisting of motor performance evaluation and 3T-magnetic resonance imaging data acquisition. Based on additional postsurgical motor deficits, 6 patients were classified into \"deficit group,\" and 6 others were into \"no deficit group.\" Using resting-state functional magnetic resonance imaging (fMRI), the integrity of functional connectivity was evaluated by placing a seed in the ipsilesional primary motor area (M1). With motor task fMRI, hand and foot representations were identified in the M1 and lateral and medial PMs. Probabilistic tractography assessed anatomic connectivity in the cortico-cortical and corticofugal networks.</p><p><strong>Results: </strong>Functional connectivity among M1 and lateral and medial PMs during resting-state fMRI was reduced postoperatively in the deficit group (<i>P</i> < .05, corrected) and preserved in the no deficit group. The deficit was unlikely to be attributable to surgical resection of specific anatomic connectivity. The amplitude of motor-evoked potential was maintained in available cases. These intraoperative observations agree with imaging findings suggesting preserved anatomic connectivity of the estimated corticofugal pathway.</p><p><strong>Conclusion: </strong>The present findings suggest that supplementary motor area syndrome is caused by disorganization of functional connectivity among cortical motor networks rather than resection of anatomic connectivity of corticofugal pathway.</p>","PeriodicalId":93342,"journal":{"name":"Neurosurgery open","volume":"1 1","pages":"e00028"},"PeriodicalIF":0.0000,"publicationDate":"2023-02-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11809952/pdf/","citationCount":"0","resultStr":"{\"title\":\"Changes in Distributed Motor Network Connectivity Correlates With Functional Outcome After Surgical Resection of Brain Tumors.\",\"authors\":\"Yukihiro Yamao, Nobukatsu Sawamoto, Takeharu Kunieda, Rika Inano, Sumiya Shibata, Takayuki Kikuchi, Yoshiki Arakawa, Kazumichi Yoshida, Riki Matsumoto, Akio Ikeda, Ryosuke Takahashi, Hidenao Fukuyama, Susumu Miyamoto\",\"doi\":\"10.1227/neuprac.0000000000000028\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In patients with brain tumors around the motor cortices, deterioration of motor performance may be observed even if the integrity of the cortical output is maintained. Especially, resection of medial premotor area (PM) can cause postoperative deterioration called supplementary motor area syndrome.</p><p><strong>Objective: </strong>To clarify the neuronal mechanisms underlying postsurgical deterioration with a case-control study.</p><p><strong>Methods: </strong>Twelve patients with brain tumors underwent preoperative and postoperative sessions consisting of motor performance evaluation and 3T-magnetic resonance imaging data acquisition. Based on additional postsurgical motor deficits, 6 patients were classified into \\\"deficit group,\\\" and 6 others were into \\\"no deficit group.\\\" Using resting-state functional magnetic resonance imaging (fMRI), the integrity of functional connectivity was evaluated by placing a seed in the ipsilesional primary motor area (M1). With motor task fMRI, hand and foot representations were identified in the M1 and lateral and medial PMs. Probabilistic tractography assessed anatomic connectivity in the cortico-cortical and corticofugal networks.</p><p><strong>Results: </strong>Functional connectivity among M1 and lateral and medial PMs during resting-state fMRI was reduced postoperatively in the deficit group (<i>P</i> < .05, corrected) and preserved in the no deficit group. The deficit was unlikely to be attributable to surgical resection of specific anatomic connectivity. The amplitude of motor-evoked potential was maintained in available cases. These intraoperative observations agree with imaging findings suggesting preserved anatomic connectivity of the estimated corticofugal pathway.</p><p><strong>Conclusion: </strong>The present findings suggest that supplementary motor area syndrome is caused by disorganization of functional connectivity among cortical motor networks rather than resection of anatomic connectivity of corticofugal pathway.</p>\",\"PeriodicalId\":93342,\"journal\":{\"name\":\"Neurosurgery open\",\"volume\":\"1 1\",\"pages\":\"e00028\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-02-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11809952/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurosurgery open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1227/neuprac.0000000000000028\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurosurgery open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1227/neuprac.0000000000000028","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Changes in Distributed Motor Network Connectivity Correlates With Functional Outcome After Surgical Resection of Brain Tumors.
Background: In patients with brain tumors around the motor cortices, deterioration of motor performance may be observed even if the integrity of the cortical output is maintained. Especially, resection of medial premotor area (PM) can cause postoperative deterioration called supplementary motor area syndrome.
Objective: To clarify the neuronal mechanisms underlying postsurgical deterioration with a case-control study.
Methods: Twelve patients with brain tumors underwent preoperative and postoperative sessions consisting of motor performance evaluation and 3T-magnetic resonance imaging data acquisition. Based on additional postsurgical motor deficits, 6 patients were classified into "deficit group," and 6 others were into "no deficit group." Using resting-state functional magnetic resonance imaging (fMRI), the integrity of functional connectivity was evaluated by placing a seed in the ipsilesional primary motor area (M1). With motor task fMRI, hand and foot representations were identified in the M1 and lateral and medial PMs. Probabilistic tractography assessed anatomic connectivity in the cortico-cortical and corticofugal networks.
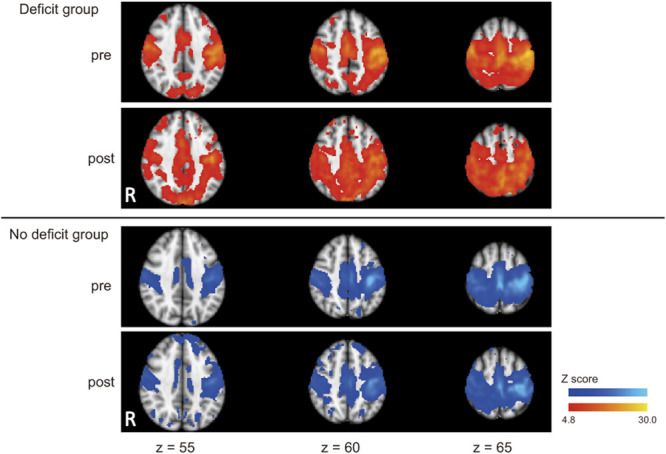
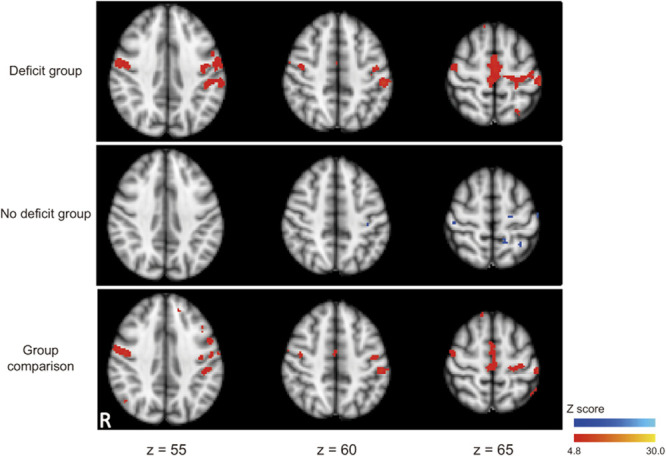
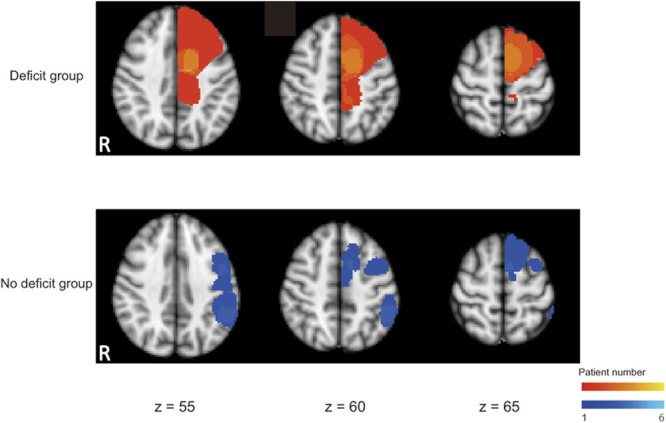
Results: Functional connectivity among M1 and lateral and medial PMs during resting-state fMRI was reduced postoperatively in the deficit group (P < .05, corrected) and preserved in the no deficit group. The deficit was unlikely to be attributable to surgical resection of specific anatomic connectivity. The amplitude of motor-evoked potential was maintained in available cases. These intraoperative observations agree with imaging findings suggesting preserved anatomic connectivity of the estimated corticofugal pathway.
Conclusion: The present findings suggest that supplementary motor area syndrome is caused by disorganization of functional connectivity among cortical motor networks rather than resection of anatomic connectivity of corticofugal pathway.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
