Charlotte Van Laeken, Thibault Taelman, Sarah Cappuyns, Geert Maleux, Vincent Vandecaveye, Chris Verslype, Christophe Deroose, Jeroen Dekervel
{"title":"肝细胞癌放射栓塞术后早期疾病进展的相关临床因素及进展后全身治疗的可行性","authors":"Charlotte Van Laeken, Thibault Taelman, Sarah Cappuyns, Geert Maleux, Vincent Vandecaveye, Chris Verslype, Christophe Deroose, Jeroen Dekervel","doi":"10.1002/lci2.60","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background and Aims</h3>\n \n <p>Radioembolization (RE) for unresectable hepatocellular carcinoma (HCC) can provide clinical benefit for well-selected patients, whilst in others, rapid disease progression is observed. As an alternative for this patient population, new potent systemic treatment options are emerging. We aimed to identify the clinical factors associated with rapid progression following RE and assess the feasibility of starting a systemic treatment after progression.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A retrospective cohort study of patients with unresectable HCC undergoing RE at a single referral centre between January 2009 and December 2018. Progression-free and overall survival times were calculated. Uni- and multivariate cox regression analysis was used to assess factors associated with poor outcomes. Charts were reviewed for post-progression treatment strategies.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Overall, 116 patients with unresectable HCC were included. Median PFS after RE was 6.7 months (95% CI 3.97–9.37), which varied significantly (<i>P</i> < .001) with Eastern Cooperative Oncology Group Performance Status (EGOC PS) (ECOG 0, 20.9 months [95% CI 8.6–33.2]; ECOG 1, 7.7 months [95% CI 3.1–12.1]; ECOG 2, 4.4 months [95% CI 1.7–7]). This association remained significant after multivariate testing, together with the number of HCC lesions (<i>P</i> = .017) and α-FP (<i>P</i> = .050). Progressive disease after RE occurred in 82 patients, of whom only 40 received subsequent systemic treatment. Again, ECOG PS at the time of progression was significantly better for patients who did receive systemic treatment versus those who did not (<i>P</i> = .002).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Patients with unresectable HCC, impaired general condition and multinodular disease have inferior outcomes after radioembolization. After RE, close monitoring of patient performance status, liver function and cancer control is warranted to allow timely initiation of systemic treatment when indicated.</p>\n </section>\n </div>","PeriodicalId":93331,"journal":{"name":"Liver cancer international","volume":"3 3","pages":"128-136"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/lci2.60","citationCount":"0","resultStr":"{\"title\":\"Clinical factors associated with early disease progression after radioembolization for hepatocellular carcinoma and feasibility of post-progression systemic therapy\",\"authors\":\"Charlotte Van Laeken, Thibault Taelman, Sarah Cappuyns, Geert Maleux, Vincent Vandecaveye, Chris Verslype, Christophe Deroose, Jeroen Dekervel\",\"doi\":\"10.1002/lci2.60\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background and Aims</h3>\\n \\n <p>Radioembolization (RE) for unresectable hepatocellular carcinoma (HCC) can provide clinical benefit for well-selected patients, whilst in others, rapid disease progression is observed. As an alternative for this patient population, new potent systemic treatment options are emerging. We aimed to identify the clinical factors associated with rapid progression following RE and assess the feasibility of starting a systemic treatment after progression.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>A retrospective cohort study of patients with unresectable HCC undergoing RE at a single referral centre between January 2009 and December 2018. Progression-free and overall survival times were calculated. Uni- and multivariate cox regression analysis was used to assess factors associated with poor outcomes. Charts were reviewed for post-progression treatment strategies.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Overall, 116 patients with unresectable HCC were included. Median PFS after RE was 6.7 months (95% CI 3.97–9.37), which varied significantly (<i>P</i> < .001) with Eastern Cooperative Oncology Group Performance Status (EGOC PS) (ECOG 0, 20.9 months [95% CI 8.6–33.2]; ECOG 1, 7.7 months [95% CI 3.1–12.1]; ECOG 2, 4.4 months [95% CI 1.7–7]). This association remained significant after multivariate testing, together with the number of HCC lesions (<i>P</i> = .017) and α-FP (<i>P</i> = .050). Progressive disease after RE occurred in 82 patients, of whom only 40 received subsequent systemic treatment. Again, ECOG PS at the time of progression was significantly better for patients who did receive systemic treatment versus those who did not (<i>P</i> = .002).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Patients with unresectable HCC, impaired general condition and multinodular disease have inferior outcomes after radioembolization. After RE, close monitoring of patient performance status, liver function and cancer control is warranted to allow timely initiation of systemic treatment when indicated.</p>\\n </section>\\n </div>\",\"PeriodicalId\":93331,\"journal\":{\"name\":\"Liver cancer international\",\"volume\":\"3 3\",\"pages\":\"128-136\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-10-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/lci2.60\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Liver cancer international\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/lci2.60\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Liver cancer international","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/lci2.60","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景与目的放射栓塞(RE)治疗不可切除的肝细胞癌(HCC)可以为选定的患者提供临床益处,而在其他患者中,观察到疾病的快速进展。作为这一患者群体的替代方案,新的有效的全身治疗方案正在出现。我们的目的是确定与RE后快速进展相关的临床因素,并评估进展后开始全身治疗的可行性。方法回顾性队列研究2009年1月至2018年12月在单个转诊中心接受RE治疗的不可切除HCC患者。计算无进展生存时间和总生存时间。采用单因素和多因素cox回归分析评估与不良预后相关的因素。回顾了进展后治疗策略的图表。结果共纳入116例不可切除HCC患者。RE后的中位PFS为6.7个月(95% CI 3.97-9.37),与东部肿瘤合作组绩效状态(ECOG) (ECOG 0, 20.9个月[95% CI 8.6-33.2];ECOG 1,7.7个月[95% CI 3.1-12.1];ECOG 2, 4.4个月[95% CI 1.7-7])。在多变量检验后,这种关联仍然显著,包括HCC病变数量(P = 0.017)和α-FP (P = 0.050)。82例患者发生RE后的进展性疾病,其中只有40例接受了后续的全身治疗。同样,接受全身治疗的患者在进展时的ECOG PS明显优于未接受全身治疗的患者(P = 0.002)。结论不可切除的肝细胞癌、全身功能受损及多结节病变患者行放射栓塞治疗后预后较差。RE术后,应密切监测患者的身体状况、肝功能和癌症控制情况,以便在需要时及时开始全身治疗。
Clinical factors associated with early disease progression after radioembolization for hepatocellular carcinoma and feasibility of post-progression systemic therapy
Background and Aims
Radioembolization (RE) for unresectable hepatocellular carcinoma (HCC) can provide clinical benefit for well-selected patients, whilst in others, rapid disease progression is observed. As an alternative for this patient population, new potent systemic treatment options are emerging. We aimed to identify the clinical factors associated with rapid progression following RE and assess the feasibility of starting a systemic treatment after progression.
Methods
A retrospective cohort study of patients with unresectable HCC undergoing RE at a single referral centre between January 2009 and December 2018. Progression-free and overall survival times were calculated. Uni- and multivariate cox regression analysis was used to assess factors associated with poor outcomes. Charts were reviewed for post-progression treatment strategies.
Results
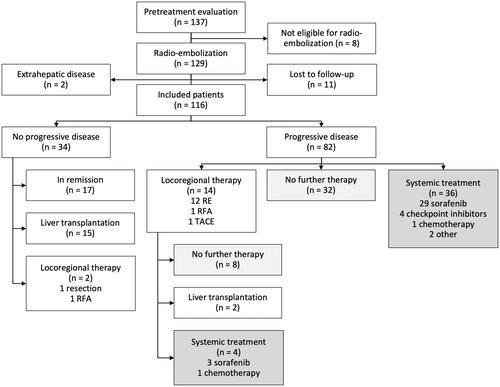
Overall, 116 patients with unresectable HCC were included. Median PFS after RE was 6.7 months (95% CI 3.97–9.37), which varied significantly (P < .001) with Eastern Cooperative Oncology Group Performance Status (EGOC PS) (ECOG 0, 20.9 months [95% CI 8.6–33.2]; ECOG 1, 7.7 months [95% CI 3.1–12.1]; ECOG 2, 4.4 months [95% CI 1.7–7]). This association remained significant after multivariate testing, together with the number of HCC lesions (P = .017) and α-FP (P = .050). Progressive disease after RE occurred in 82 patients, of whom only 40 received subsequent systemic treatment. Again, ECOG PS at the time of progression was significantly better for patients who did receive systemic treatment versus those who did not (P = .002).
Conclusion
Patients with unresectable HCC, impaired general condition and multinodular disease have inferior outcomes after radioembolization. After RE, close monitoring of patient performance status, liver function and cancer control is warranted to allow timely initiation of systemic treatment when indicated.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
