Ehab Hanafy Shaker, Ahmed Mohamed Soliman, Ahmed Fahmy Hussein, Ehab Samy Fayek, Mai Mohamed Elrawas
{"title":"评估单剂量氨甲环酸在减少细胞减少手术后高温腹腔化疗期间失血的有效性和安全性:一项随机比较先导研究","authors":"Ehab Hanafy Shaker, Ahmed Mohamed Soliman, Ahmed Fahmy Hussein, Ehab Samy Fayek, Mai Mohamed Elrawas","doi":"10.5812/aapm-136578","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hyperthermic intraperitoneal chemotherapy (HIPEC), following cytoreductive surgery (CRS), is a lengthy procedure, usually associated with considerable bleeding due to the extensive nature of surgery. Various techniques have been used to decrease blood transfusion requirements.</p><p><strong>Objectives: </strong>This study aimed to evaluate the possible advantage of a single dose of tranexamic acid (TA) in such surgeries.</p><p><strong>Methods: </strong>In this randomized comparative pilot study, 60 patients scheduled to undergo CRS followed by HIPEC were randomly assigned to 2 equal groups: group 1 (TA group) that received 10 mg/kg of TA in 100 mL of 0.9% NaCl over 20 minutes after the induction of anesthesia and before surgical incision, and group 2 (control group) that received a placebo of 100 mL of 0.9% NaCl during the same time interval. The primary endpoint was the blood loss volume. The secondary endpoints were the number of patients requiring transfusion and the occurrence of any postoperative thrombotic events 30 days after surgery. Serum creatinine levels were measured before the operation and on postoperative days 1, 3, and 5. Intraoperative and first 24 hours urine outputs were also recorded. The levels of hemoglobin (Hb) were measured before the operation, immediately after the operation, and 5 days postoperatively.</p><p><strong>Results: </strong>Compared to the control group, the TA group exhibited lower intraoperative blood loss, as well as lower blood loss on postoperative day 1 and in total blood loss (P = 0.006, 0.035, and 0.001, respectively). However, the blood loss on the remaining postoperative days was comparable between both groups. Intraoperative blood transfusion requirements were lower in the TA group (P = 0.032) than in the control group. The total number of units of blood and plasma transfused was also lower in the TA group both intra and postoperatively (0.007, 0.40, and 0.032, 0.008, respectively) than in the control group. Hemoglobin levels, serum creatinine levels, and urine outputs during the first 24 hours postoperatively were comparable between the 2 groups. The thromboembolic events within 30 days were also comparable between the 2 groups.</p><p><strong>Conclusions: </strong>Administering a single dose of TA between the induction of anesthesia and the surgical incision may reduce blood loss and transfusion rates in CRS followed by HIPEC without causing significant adverse effects. It is a promising approach in surgeries where massive blood loss is expected shortly after anesthesia induction. This can minimize the drawbacks of repeated blood transfusions during and after the operation without causing significant adverse effects. Besides reducing the need for repeated blood transfusions, it would also reduce the costs of blood/blood products and the risks of transfusion.</p>","PeriodicalId":7841,"journal":{"name":"Anesthesiology and Pain Medicine","volume":" ","pages":"e136578"},"PeriodicalIF":0.0000,"publicationDate":"2023-07-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10664172/pdf/","citationCount":"0","resultStr":"{\"title\":\"Evaluating the Efficacy and Safety of a Single-Dose Tranexamic Acid in Reducing Blood Loss During Cytoreductive Surgery Followed by Hyperthermic Intraperitoneal Chemotherapy: A Randomized Comparative Pilot Study.\",\"authors\":\"Ehab Hanafy Shaker, Ahmed Mohamed Soliman, Ahmed Fahmy Hussein, Ehab Samy Fayek, Mai Mohamed Elrawas\",\"doi\":\"10.5812/aapm-136578\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Hyperthermic intraperitoneal chemotherapy (HIPEC), following cytoreductive surgery (CRS), is a lengthy procedure, usually associated with considerable bleeding due to the extensive nature of surgery. Various techniques have been used to decrease blood transfusion requirements.</p><p><strong>Objectives: </strong>This study aimed to evaluate the possible advantage of a single dose of tranexamic acid (TA) in such surgeries.</p><p><strong>Methods: </strong>In this randomized comparative pilot study, 60 patients scheduled to undergo CRS followed by HIPEC were randomly assigned to 2 equal groups: group 1 (TA group) that received 10 mg/kg of TA in 100 mL of 0.9% NaCl over 20 minutes after the induction of anesthesia and before surgical incision, and group 2 (control group) that received a placebo of 100 mL of 0.9% NaCl during the same time interval. The primary endpoint was the blood loss volume. The secondary endpoints were the number of patients requiring transfusion and the occurrence of any postoperative thrombotic events 30 days after surgery. Serum creatinine levels were measured before the operation and on postoperative days 1, 3, and 5. Intraoperative and first 24 hours urine outputs were also recorded. The levels of hemoglobin (Hb) were measured before the operation, immediately after the operation, and 5 days postoperatively.</p><p><strong>Results: </strong>Compared to the control group, the TA group exhibited lower intraoperative blood loss, as well as lower blood loss on postoperative day 1 and in total blood loss (P = 0.006, 0.035, and 0.001, respectively). However, the blood loss on the remaining postoperative days was comparable between both groups. Intraoperative blood transfusion requirements were lower in the TA group (P = 0.032) than in the control group. The total number of units of blood and plasma transfused was also lower in the TA group both intra and postoperatively (0.007, 0.40, and 0.032, 0.008, respectively) than in the control group. Hemoglobin levels, serum creatinine levels, and urine outputs during the first 24 hours postoperatively were comparable between the 2 groups. The thromboembolic events within 30 days were also comparable between the 2 groups.</p><p><strong>Conclusions: </strong>Administering a single dose of TA between the induction of anesthesia and the surgical incision may reduce blood loss and transfusion rates in CRS followed by HIPEC without causing significant adverse effects. It is a promising approach in surgeries where massive blood loss is expected shortly after anesthesia induction. This can minimize the drawbacks of repeated blood transfusions during and after the operation without causing significant adverse effects. Besides reducing the need for repeated blood transfusions, it would also reduce the costs of blood/blood products and the risks of transfusion.</p>\",\"PeriodicalId\":7841,\"journal\":{\"name\":\"Anesthesiology and Pain Medicine\",\"volume\":\" \",\"pages\":\"e136578\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-07-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10664172/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Anesthesiology and Pain Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5812/aapm-136578\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/8/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesiology and Pain Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5812/aapm-136578","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
背景:细胞减缩手术(CRS)后的高温腹腔化疗(HIPEC)是一个漫长的过程,由于手术的广泛性,通常伴有大量出血。已经使用了各种技术来减少输血需求。目的:本研究旨在评估单剂量氨甲环酸(TA)在此类手术中的可能优势。方法:在这项随机对照先导研究中,60例计划接受CRS和HIPEC的患者被随机分为两组:1组(TA组)在麻醉诱导后和手术切口前20分钟内接受100 mL 0.9% NaCl中10 mg/kg TA, 2组(对照组)在相同的时间间隔内接受100 mL 0.9% NaCl的安慰剂。主要终点是失血量。次要终点是需要输血的患者数量和术后30天血栓事件的发生。术前及术后第1、3、5天测定血清肌酐水平。同时记录术中及前24小时的尿量。分别于术前、术后及术后5 d测定血红蛋白(Hb)水平。结果:与对照组相比,TA组术中出血量更低,术后第1天出血量和总出血量更低(P分别为0.006、0.035和0.001)。然而,两组术后剩余几天的出血量是相当的。TA组术中输血需要量低于对照组(P = 0.032)。TA组术中、术后输血总单位数均低于对照组(分别为0.007、0.40和0.032、0.008)。两组患者术后24小时血红蛋白水平、血清肌酐水平和尿量具有可比性。30天内的血栓栓塞事件在两组之间也具有可比性。结论:在麻醉诱导和手术切口之间给予单剂量TA可减少CRS术后HIPEC的出血量和输血率,且不会引起明显的不良反应。这是一种很有前途的手术方法,在麻醉诱导后不久预计会大量失血。这可以最大限度地减少手术期间和手术后反复输血的缺点,而不会引起明显的不良反应。除了减少反复输血的需要外,它还将降低血液/血液制品的成本和输血的风险。
Evaluating the Efficacy and Safety of a Single-Dose Tranexamic Acid in Reducing Blood Loss During Cytoreductive Surgery Followed by Hyperthermic Intraperitoneal Chemotherapy: A Randomized Comparative Pilot Study.
Background: Hyperthermic intraperitoneal chemotherapy (HIPEC), following cytoreductive surgery (CRS), is a lengthy procedure, usually associated with considerable bleeding due to the extensive nature of surgery. Various techniques have been used to decrease blood transfusion requirements.
Objectives: This study aimed to evaluate the possible advantage of a single dose of tranexamic acid (TA) in such surgeries.
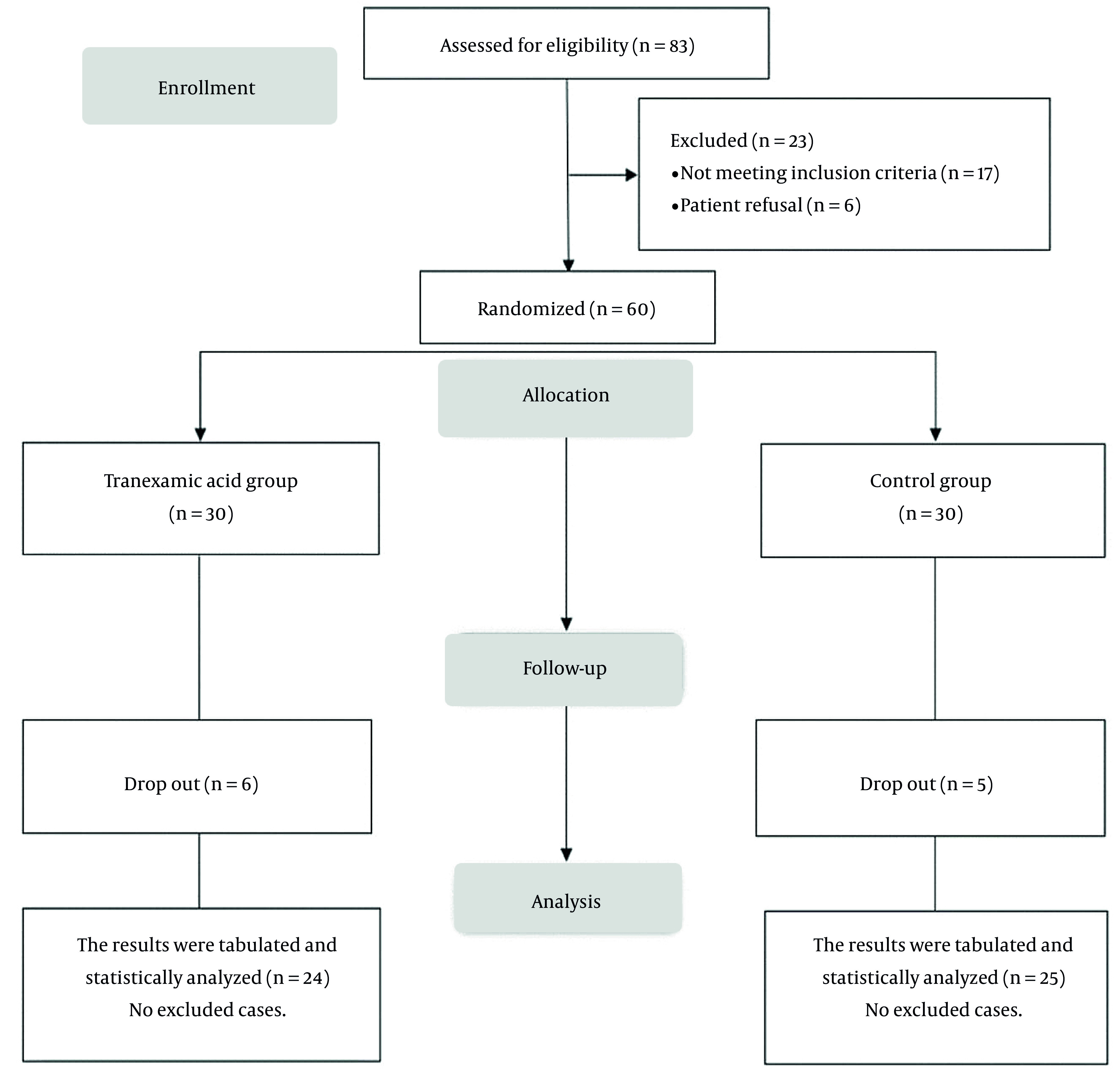
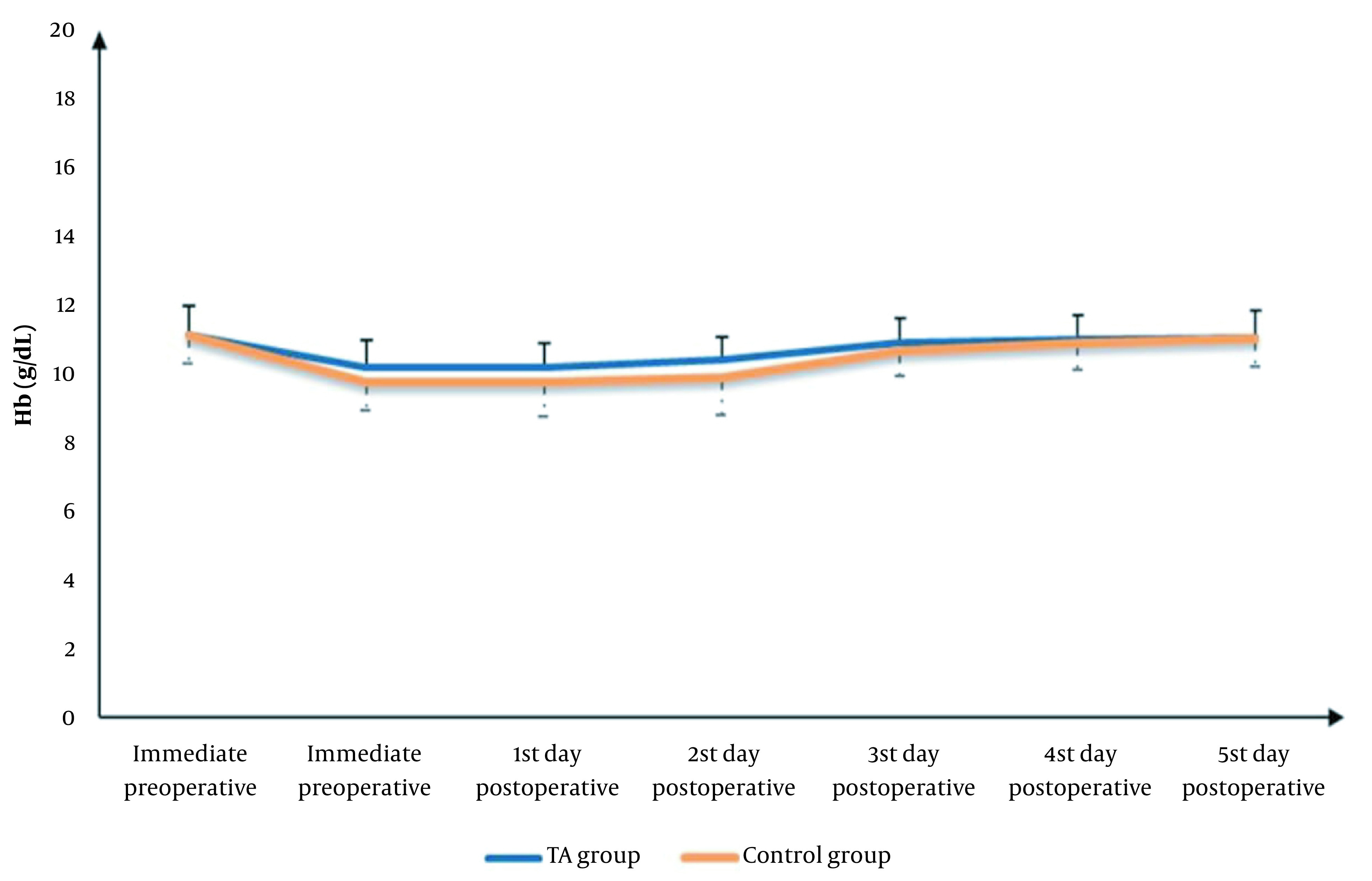
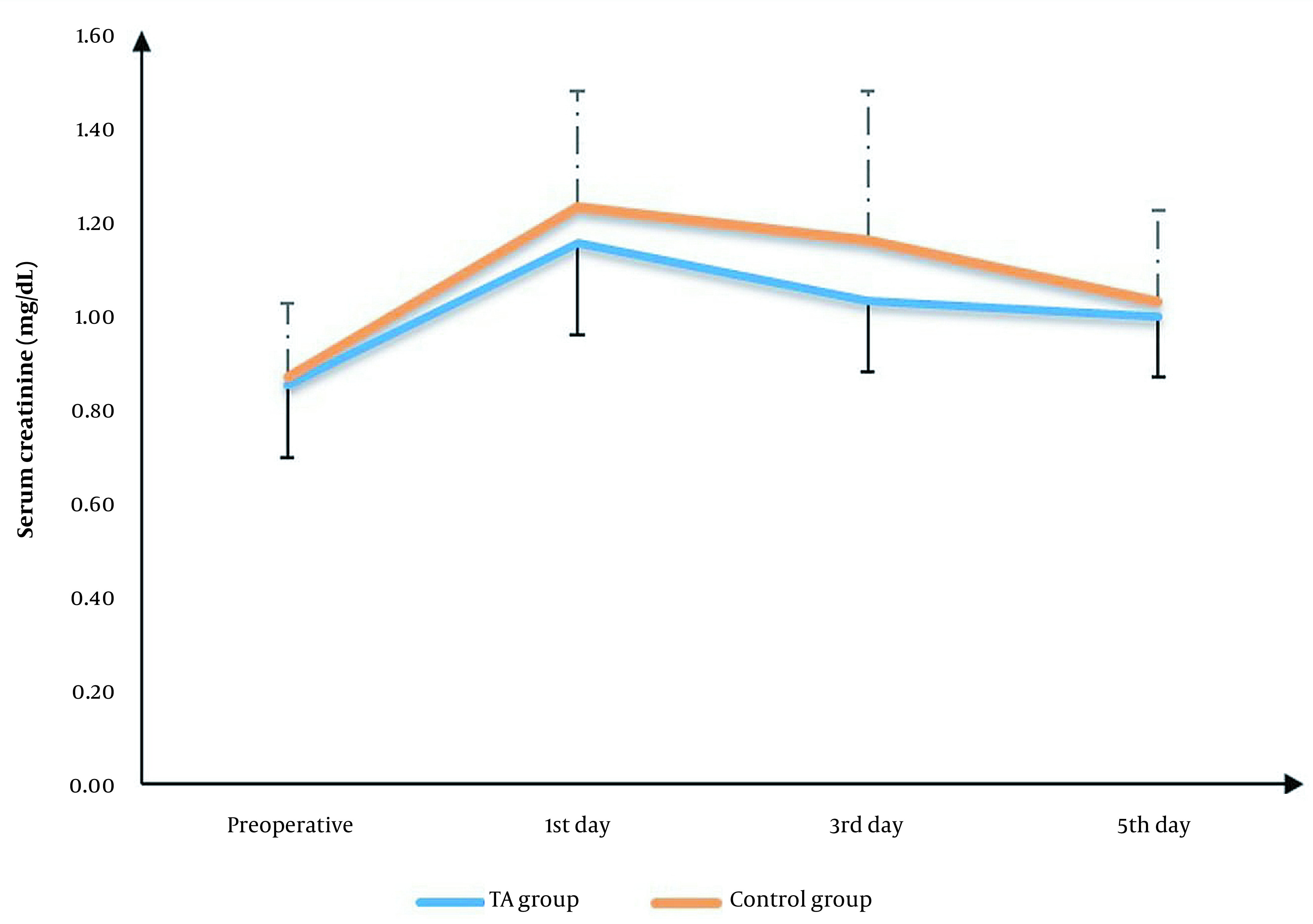
Methods: In this randomized comparative pilot study, 60 patients scheduled to undergo CRS followed by HIPEC were randomly assigned to 2 equal groups: group 1 (TA group) that received 10 mg/kg of TA in 100 mL of 0.9% NaCl over 20 minutes after the induction of anesthesia and before surgical incision, and group 2 (control group) that received a placebo of 100 mL of 0.9% NaCl during the same time interval. The primary endpoint was the blood loss volume. The secondary endpoints were the number of patients requiring transfusion and the occurrence of any postoperative thrombotic events 30 days after surgery. Serum creatinine levels were measured before the operation and on postoperative days 1, 3, and 5. Intraoperative and first 24 hours urine outputs were also recorded. The levels of hemoglobin (Hb) were measured before the operation, immediately after the operation, and 5 days postoperatively.
Results: Compared to the control group, the TA group exhibited lower intraoperative blood loss, as well as lower blood loss on postoperative day 1 and in total blood loss (P = 0.006, 0.035, and 0.001, respectively). However, the blood loss on the remaining postoperative days was comparable between both groups. Intraoperative blood transfusion requirements were lower in the TA group (P = 0.032) than in the control group. The total number of units of blood and plasma transfused was also lower in the TA group both intra and postoperatively (0.007, 0.40, and 0.032, 0.008, respectively) than in the control group. Hemoglobin levels, serum creatinine levels, and urine outputs during the first 24 hours postoperatively were comparable between the 2 groups. The thromboembolic events within 30 days were also comparable between the 2 groups.
Conclusions: Administering a single dose of TA between the induction of anesthesia and the surgical incision may reduce blood loss and transfusion rates in CRS followed by HIPEC without causing significant adverse effects. It is a promising approach in surgeries where massive blood loss is expected shortly after anesthesia induction. This can minimize the drawbacks of repeated blood transfusions during and after the operation without causing significant adverse effects. Besides reducing the need for repeated blood transfusions, it would also reduce the costs of blood/blood products and the risks of transfusion.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
