{"title":"一名患有亚急性脑病、肌阵挛和退行性变的三岁女孩","authors":"Shermila Pia, Ryan Carrier, David Bearden","doi":"10.1002/cns3.20037","DOIUrl":null,"url":null,"abstract":"<p>This previously healthy three-year-old girl presented with two months of developmental regression, progressive fatigue, and jerking movements in the setting of failure to thrive and macrocytic anemia. She previously spoke in full sentences but began using only one-to-two-word phrases. She would collapse after walking short distances or going up stairs. Examination revealed lethargy, irritability, myoclonic jerks of trunk and limbs, diffuse hyperreflexia with clonus, and wide-based unsteady gait. Labs showed vitamin B<sub>12</sub> < 200 pg/mL (lowest reportable), methylmalonic acid 14 μmol/L (ref. 0.0–0.4 μmol/L), homocysteine 224 μmol/L (ref. 0–15 μmol/L), and mean corpuscular volume 110 (ref. 76–87 fL). Magnetic resonance imaging revealed no brain abnormalities, but spinal imaging showed extensive T2 hyperintensity of the dorsal columns (Figure 1). She was diagnosed with spinal cord degeneration secondary to vitamin B<sub>12</sub> deficiency. Parenteral B<sub>12</sub> supplementation led to rapid clinical improvement. However, without continued parenteral supplementation, she had declining B<sub>12</sub> levels and is undergoing further investigation for a malabsorptive or genetic-metabolic etiology.</p><p>Cobalamin, or vitamin B<sub>12</sub>, is important in myelin metabolism and brain development. Pediatric B<sub>12</sub> deficiency is most commonly due to nutritional insufficiency, malabsorption, or more rarely, genetic-metabolic syndromes.<span><sup>1-3</sup></span> Infants and toddlers often present with developmental regression, lethargy, hypotonia, and abnormal movements such as myoclonus or chorea.<span><sup>1, 4</sup></span> Spinal cord degeneration secondary to B<sub>12</sub> deficiency is exceedingly rare in children in developed countries.<span><sup>1, 2</sup></span> In terms of treatment, oral B<sub>12</sub> replacement is sufficient in cases of nutritional deficiency. Malabsorptive or genetic-metabolic etiologies, on the other hand, are likely to require ongoing parenteral supplementation.<span><sup>3</sup></span> Prognosis is dependent on age of onset and duration of uncorrected B<sub>12</sub> deficiency.<span><sup>1</sup></span></p><p><b>Shermila Pia</b>: Conceptualization; investigation; writing—original draft. <b>Ryan Carrier</b>: Writing—review & editing. <b>David Bearden</b>: Supervision; writing—review & editing.</p><p>DB is an associate editor for <i>Annals of the Child Neurology Society</i>. SP and RC declare no conflicts of interest.</p>","PeriodicalId":72232,"journal":{"name":"Annals of the Child Neurology Society","volume":"1 3","pages":"254-255"},"PeriodicalIF":0.0000,"publicationDate":"2023-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cns3.20037","citationCount":"0","resultStr":"{\"title\":\"A three-year-old girl with subacute encephalopathy, myoclonus, and regression\",\"authors\":\"Shermila Pia, Ryan Carrier, David Bearden\",\"doi\":\"10.1002/cns3.20037\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>This previously healthy three-year-old girl presented with two months of developmental regression, progressive fatigue, and jerking movements in the setting of failure to thrive and macrocytic anemia. She previously spoke in full sentences but began using only one-to-two-word phrases. She would collapse after walking short distances or going up stairs. Examination revealed lethargy, irritability, myoclonic jerks of trunk and limbs, diffuse hyperreflexia with clonus, and wide-based unsteady gait. Labs showed vitamin B<sub>12</sub> < 200 pg/mL (lowest reportable), methylmalonic acid 14 μmol/L (ref. 0.0–0.4 μmol/L), homocysteine 224 μmol/L (ref. 0–15 μmol/L), and mean corpuscular volume 110 (ref. 76–87 fL). Magnetic resonance imaging revealed no brain abnormalities, but spinal imaging showed extensive T2 hyperintensity of the dorsal columns (Figure 1). She was diagnosed with spinal cord degeneration secondary to vitamin B<sub>12</sub> deficiency. Parenteral B<sub>12</sub> supplementation led to rapid clinical improvement. However, without continued parenteral supplementation, she had declining B<sub>12</sub> levels and is undergoing further investigation for a malabsorptive or genetic-metabolic etiology.</p><p>Cobalamin, or vitamin B<sub>12</sub>, is important in myelin metabolism and brain development. Pediatric B<sub>12</sub> deficiency is most commonly due to nutritional insufficiency, malabsorption, or more rarely, genetic-metabolic syndromes.<span><sup>1-3</sup></span> Infants and toddlers often present with developmental regression, lethargy, hypotonia, and abnormal movements such as myoclonus or chorea.<span><sup>1, 4</sup></span> Spinal cord degeneration secondary to B<sub>12</sub> deficiency is exceedingly rare in children in developed countries.<span><sup>1, 2</sup></span> In terms of treatment, oral B<sub>12</sub> replacement is sufficient in cases of nutritional deficiency. Malabsorptive or genetic-metabolic etiologies, on the other hand, are likely to require ongoing parenteral supplementation.<span><sup>3</sup></span> Prognosis is dependent on age of onset and duration of uncorrected B<sub>12</sub> deficiency.<span><sup>1</sup></span></p><p><b>Shermila Pia</b>: Conceptualization; investigation; writing—original draft. <b>Ryan Carrier</b>: Writing—review & editing. <b>David Bearden</b>: Supervision; writing—review & editing.</p><p>DB is an associate editor for <i>Annals of the Child Neurology Society</i>. SP and RC declare no conflicts of interest.</p>\",\"PeriodicalId\":72232,\"journal\":{\"name\":\"Annals of the Child Neurology Society\",\"volume\":\"1 3\",\"pages\":\"254-255\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-08-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cns3.20037\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of the Child Neurology Society\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cns3.20037\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of the Child Neurology Society","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cns3.20037","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
A three-year-old girl with subacute encephalopathy, myoclonus, and regression
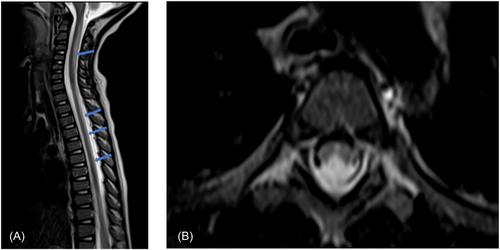
This previously healthy three-year-old girl presented with two months of developmental regression, progressive fatigue, and jerking movements in the setting of failure to thrive and macrocytic anemia. She previously spoke in full sentences but began using only one-to-two-word phrases. She would collapse after walking short distances or going up stairs. Examination revealed lethargy, irritability, myoclonic jerks of trunk and limbs, diffuse hyperreflexia with clonus, and wide-based unsteady gait. Labs showed vitamin B12 < 200 pg/mL (lowest reportable), methylmalonic acid 14 μmol/L (ref. 0.0–0.4 μmol/L), homocysteine 224 μmol/L (ref. 0–15 μmol/L), and mean corpuscular volume 110 (ref. 76–87 fL). Magnetic resonance imaging revealed no brain abnormalities, but spinal imaging showed extensive T2 hyperintensity of the dorsal columns (Figure 1). She was diagnosed with spinal cord degeneration secondary to vitamin B12 deficiency. Parenteral B12 supplementation led to rapid clinical improvement. However, without continued parenteral supplementation, she had declining B12 levels and is undergoing further investigation for a malabsorptive or genetic-metabolic etiology.
Cobalamin, or vitamin B12, is important in myelin metabolism and brain development. Pediatric B12 deficiency is most commonly due to nutritional insufficiency, malabsorption, or more rarely, genetic-metabolic syndromes.1-3 Infants and toddlers often present with developmental regression, lethargy, hypotonia, and abnormal movements such as myoclonus or chorea.1, 4 Spinal cord degeneration secondary to B12 deficiency is exceedingly rare in children in developed countries.1, 2 In terms of treatment, oral B12 replacement is sufficient in cases of nutritional deficiency. Malabsorptive or genetic-metabolic etiologies, on the other hand, are likely to require ongoing parenteral supplementation.3 Prognosis is dependent on age of onset and duration of uncorrected B12 deficiency.1
Shermila Pia: Conceptualization; investigation; writing—original draft. Ryan Carrier: Writing—review & editing. David Bearden: Supervision; writing—review & editing.
DB is an associate editor for Annals of the Child Neurology Society. SP and RC declare no conflicts of interest.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
