Richard Pinder, Linda Bauld, Hannah Findlater, Abinav Mohanamurali, Ann Johnson, Fraser Birrell
{"title":"是时候将生活方式医学纳入本科和研究生课程了吗?","authors":"Richard Pinder, Linda Bauld, Hannah Findlater, Abinav Mohanamurali, Ann Johnson, Fraser Birrell","doi":"10.1002/lim2.59","DOIUrl":null,"url":null,"abstract":"<p>Some light at the end of the COVID-19 tunnel may be nearing. Yet, that same light is revealing a larger and longer term burden on our communities. Our educational institutions and health services have not been spared. The pandemic has catalysed the longer standing impact of anxiety, stress and burnout for many frontline health workers and younger people in particular. It has magnified socioeconomic and wider inequalities that are so detrimental to health and well-being.</p><p>While fiscal responses to the pandemic continue to be debated, there remains a fundamental barrier for the triad of Public Health, Social Care and Health Care resourcing: workforce. The historical absence of strategic workforce planning in the United Kingdom's National Health Services means that without extending (ethically challenging) international recruitment efforts, even substantial injections of finance into health and care economies are stymied by how such monies can be spent.</p><p>Lifestyle Medicine stands ready to yield a double dividend. First: to leverage self-care and health improvement amid the plethora of contact points that our communities have with public and third sector services. And second: to protect the health of our current and future workforce. While Lifestyle Medicine is no substitute for traditional population-level public health interventions, Lifestyle Medicine is an important and scalable element of the population health armamentarium, not least as systems seek increasingly integrated and preventive approaches to health and well-being. Behaviour change in the form of physical activity has been recently highlighted as a first-line therapy by U.K. health regulators in the management of depression (National Institute for Health and Care Excellent)<span><sup>2</sup></span> and many other chronic physical health conditions. The relevance of health behaviours to mitigate communicable disease threats such as the COVID-19 pandemic will be clear in the minds of many. The need for skills in promoting lifestyle changes is endorsed as a core component of U.K. medical training.<span><sup>3</sup></span></p><p>The specialty of Lifestyle Medicine, often described as emerging, can increasingly be described as maturing. As the American College of Lifestyle Medicine (ACLM) approaches 18 years of age, and the British Society of Lifestyle Medicine (BSLM) enters its seventh year, the global governance of the movement is transitioning too, with a new World Lifestyle Medicine Council. At the same time, consensus is being achieved on the specialty's scope: six pillars of lifestyle and increasingly concrete clinical application such as coaching, behaviour change and group consultations.</p><p>The evolution of interdisciplinary areas of practice is dependent on consensus - followed by convergence of both scope and practice. And while initially that involves interdisciplinary working, the extent to which Lifestyle Medicine is a logical expansion of scope for general practitioners or hospitalists versus a core multidisciplinary set of competencies is yet to be determined. While these two approaches are by no means mutually exclusive, we propose the former is desirable and the latter is essential. For the discipline to flourish, we need to integrate explicit Lifestyle Medicine competencies in a spiral approach throughout undergraduate and postgraduate training, with additional options to specialise and develop for those in senior posts looking to extend their practice.</p><p>In the United Kingdom, the (International Board) Certification in Lifestyle Medicine is the BSLM's first foray into the postgraduate space with non-medically qualified clinicians currently achieving the qualification alongside doctors. In parallel, work is also underway to establish Lifestyle Medicine in undergraduate curricula. At the front of this charge has been the innovative Lifestyle Medicine and Prevention (LMAP) modules that now form 15% of the core first 2 years of the Imperial College School of Medicine (ICSM) curriculum.</p><p>At Imperial, the Lifestyle Medicine agenda has proven an effective vehicle for Public Health to be taught through a more clinically oriented lens. The 1968 Todd Report on medical education cited Social Medicine (a predecessor to Public Health in medical curricula) as being ‘dull, neither useful nor difficult’. Few senior clinicians recall memories, and even fewer positive ones, of their own experience of Public Health during medical school.</p><p>Population Health is a broader term including public health medicine and wider disciplines (including non-medical interventions) that describes the amount of health and its distribution across a population.<span><sup>4</sup></span> At the same time, the term Lifestyle Medicine has itself been criticised for diminishing the role that structural inequalities play in determining health outcomes, not least for socioeconomically disadvantaged groups.<span><sup>5</sup></span> We argue the reverse is true. The teaching of Lifestyle Medicine (as a clinical approach) in the context of the wider determinants of health and associated inequalities (at population-level) is an avenue that can engender empathy and contextual understanding of patients’ decision-making and agency within clinical practice. Qualitative findings from two years of teaching with medical students at Imperial are already highlighting the understanding that a Lifestyle Medicine approach can establish. One student recently told us: ‘<i>Initially it was very hard to understand why some people do particular things which can lead to a detriment to their health, but this module has helped me think in their shoes, which is essential if you want to… change… behaviour</i>’.</p><p>The teaching of Lifestyle Medicine skills confers benefits for both future clinicians and the cadre of clinical teachers providing such training. Knowledge (or lack thereof) of health behaviours, guidelines and behaviour change among clinicians is cited as a reason that such initiatives are not offered in clinical consultations.<span><sup>6</sup></span></p><p>Establishing clinician knowledge on evidence-based targets for physical activity, smoking cessation, alcohol consumption, sleep or healthy eating can too easily be put into the ‘common sense’ category and disregarded amid fierce competition for curriculum space during training. Eighty percent of U.K. medical students responding to a questionnaire in 2019 (<i>N</i> = 158) reported receiving no training in Lifestyle Medicine in the most recent 2 years.<span><sup>7</sup></span> Other surveys have revealed major gaps in nutrition teaching for medics with one survey finding only 45% of respondents had received any training on nutrition and generally low levels of self-confidence in managing nutrition-related issues.<span><sup>8</sup></span> Previous surveys among medical students have found low levels of basic knowledge about smoking, due to lack of training in how to address this.<span><sup>9, 10</sup></span></p><p>Turning to the concept of the double dividend, the same knowledge and skillset that underpins clinical competence is highly relevant and applicable to self-care and burnout prevention among medical students and healthcare professionals more broadly. The growing burden of anxiety, stress and other mental health disorders are increasingly challenging to manage among medical educators, trainers and medical managers.<span><sup>11</sup></span> Lifestyle Medicine teaching is therefore a preventive intervention for workforce well-being too. At Imperial College London, students today describe their negative health behaviours as ‘not very LMAP’ demonstrating how their clinical learning is potentially influencing their own health behaviour.</p><p>For more senior clinicians fearing that teaching well-being and positive health behaviours to medical students may be patronising, such anxieties can be allayed. While Lifestyle Medicine is currently delivered at postgraduate level through the International Board of Lifestyle Medicine Certification (Figure 1), the younger generation is more in touch and non-stigmatising in how it deals and relates to concepts of well-being and mental health. Seventy-six percent of U.K. students responding to a 2018 survey wanted Lifestyle Medicine to be incorporated into the curriculum at their medical school.<span><sup>7</sup></span> The recent growth in student-driven UK Lifestyle Medicine societies (supported by BSLM) is evidence that the younger generation recognises the value the specialty can provide. Regional conferences, such as the undergraduate Lifestyle Medicine Festival of the North in February 2022, have been warmly received by students.</p><p>Lifestyle Medicine teaching is about values, skills and knowledge (Figure 1). Memorising guidelines is insufficient if the skills to apply such understanding through motivational interviewing or coaching are not similarly developed. Instilling self-efficacy and confidence to deliver Lifestyle Medicine interventions as part of the clinical consultation offers great return on investment. The skills developed in Lifestyle Medicine are broad based, scalable and relevant to most, if not all clinical interactions.</p><p>We believe Lifestyle Medicine approaches are welcomed by patients too, although the literature in this area is comparatively less developed at present. Lifestyle Medicine is usually positioned within a frame of self-efficacy drawing on ideas of shared decision-making, personalised care and self-management. The centrality of relationships and the family unit is critical: both recognising family members as enablers of lifestyle change but also potential beneficiaries when diet or addictions are addressed. Similar to the benefits that lifestyle change can provide for healthcare providers, there are opportunities for similar gains among formal and informal carers too.</p><p>The public at large, driven by patient ambassadors (such as author AJ), is the key partner in articulating the Lifestyle Medicine argument. Lay proponents are central to pre-empting cynicism that suggests addressing lifestyle translates to blame and precedes the wholesale transfer of health responsibilities to patients. Lifestyle Medicine must not become an either–or. Instead, it is a starting point, a means of sustaining and augmenting more traditional medical approaches.</p><p>Embedding Lifestyle Medicine into the skillset of all our future doctors and clinicians is an opportunity to create a virtuous cycle that improves the health of our patients and our populations and protects our workforce ahead of a challenging and uncertain future. This can assist the public health workforce in their efforts to address wider determinants of health in a range of organisations. We contend Lifestyle Medicine must become a core component of undergraduate and postgraduate medical curricula.</p><p>Editor-in-Chief Fraser Birrell is also one of the authors.</p>","PeriodicalId":74076,"journal":{"name":"Lifestyle medicine (Hoboken, N.J.)","volume":"3 2","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2022-04-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/lim2.59","citationCount":"1","resultStr":"{\"title\":\"Is it time to embed Lifestyle Medicine in undergraduate and postgraduate curricula?\",\"authors\":\"Richard Pinder, Linda Bauld, Hannah Findlater, Abinav Mohanamurali, Ann Johnson, Fraser Birrell\",\"doi\":\"10.1002/lim2.59\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Some light at the end of the COVID-19 tunnel may be nearing. Yet, that same light is revealing a larger and longer term burden on our communities. Our educational institutions and health services have not been spared. The pandemic has catalysed the longer standing impact of anxiety, stress and burnout for many frontline health workers and younger people in particular. It has magnified socioeconomic and wider inequalities that are so detrimental to health and well-being.</p><p>While fiscal responses to the pandemic continue to be debated, there remains a fundamental barrier for the triad of Public Health, Social Care and Health Care resourcing: workforce. The historical absence of strategic workforce planning in the United Kingdom's National Health Services means that without extending (ethically challenging) international recruitment efforts, even substantial injections of finance into health and care economies are stymied by how such monies can be spent.</p><p>Lifestyle Medicine stands ready to yield a double dividend. First: to leverage self-care and health improvement amid the plethora of contact points that our communities have with public and third sector services. And second: to protect the health of our current and future workforce. While Lifestyle Medicine is no substitute for traditional population-level public health interventions, Lifestyle Medicine is an important and scalable element of the population health armamentarium, not least as systems seek increasingly integrated and preventive approaches to health and well-being. Behaviour change in the form of physical activity has been recently highlighted as a first-line therapy by U.K. health regulators in the management of depression (National Institute for Health and Care Excellent)<span><sup>2</sup></span> and many other chronic physical health conditions. The relevance of health behaviours to mitigate communicable disease threats such as the COVID-19 pandemic will be clear in the minds of many. The need for skills in promoting lifestyle changes is endorsed as a core component of U.K. medical training.<span><sup>3</sup></span></p><p>The specialty of Lifestyle Medicine, often described as emerging, can increasingly be described as maturing. As the American College of Lifestyle Medicine (ACLM) approaches 18 years of age, and the British Society of Lifestyle Medicine (BSLM) enters its seventh year, the global governance of the movement is transitioning too, with a new World Lifestyle Medicine Council. At the same time, consensus is being achieved on the specialty's scope: six pillars of lifestyle and increasingly concrete clinical application such as coaching, behaviour change and group consultations.</p><p>The evolution of interdisciplinary areas of practice is dependent on consensus - followed by convergence of both scope and practice. And while initially that involves interdisciplinary working, the extent to which Lifestyle Medicine is a logical expansion of scope for general practitioners or hospitalists versus a core multidisciplinary set of competencies is yet to be determined. While these two approaches are by no means mutually exclusive, we propose the former is desirable and the latter is essential. For the discipline to flourish, we need to integrate explicit Lifestyle Medicine competencies in a spiral approach throughout undergraduate and postgraduate training, with additional options to specialise and develop for those in senior posts looking to extend their practice.</p><p>In the United Kingdom, the (International Board) Certification in Lifestyle Medicine is the BSLM's first foray into the postgraduate space with non-medically qualified clinicians currently achieving the qualification alongside doctors. In parallel, work is also underway to establish Lifestyle Medicine in undergraduate curricula. At the front of this charge has been the innovative Lifestyle Medicine and Prevention (LMAP) modules that now form 15% of the core first 2 years of the Imperial College School of Medicine (ICSM) curriculum.</p><p>At Imperial, the Lifestyle Medicine agenda has proven an effective vehicle for Public Health to be taught through a more clinically oriented lens. The 1968 Todd Report on medical education cited Social Medicine (a predecessor to Public Health in medical curricula) as being ‘dull, neither useful nor difficult’. Few senior clinicians recall memories, and even fewer positive ones, of their own experience of Public Health during medical school.</p><p>Population Health is a broader term including public health medicine and wider disciplines (including non-medical interventions) that describes the amount of health and its distribution across a population.<span><sup>4</sup></span> At the same time, the term Lifestyle Medicine has itself been criticised for diminishing the role that structural inequalities play in determining health outcomes, not least for socioeconomically disadvantaged groups.<span><sup>5</sup></span> We argue the reverse is true. The teaching of Lifestyle Medicine (as a clinical approach) in the context of the wider determinants of health and associated inequalities (at population-level) is an avenue that can engender empathy and contextual understanding of patients’ decision-making and agency within clinical practice. Qualitative findings from two years of teaching with medical students at Imperial are already highlighting the understanding that a Lifestyle Medicine approach can establish. One student recently told us: ‘<i>Initially it was very hard to understand why some people do particular things which can lead to a detriment to their health, but this module has helped me think in their shoes, which is essential if you want to… change… behaviour</i>’.</p><p>The teaching of Lifestyle Medicine skills confers benefits for both future clinicians and the cadre of clinical teachers providing such training. Knowledge (or lack thereof) of health behaviours, guidelines and behaviour change among clinicians is cited as a reason that such initiatives are not offered in clinical consultations.<span><sup>6</sup></span></p><p>Establishing clinician knowledge on evidence-based targets for physical activity, smoking cessation, alcohol consumption, sleep or healthy eating can too easily be put into the ‘common sense’ category and disregarded amid fierce competition for curriculum space during training. Eighty percent of U.K. medical students responding to a questionnaire in 2019 (<i>N</i> = 158) reported receiving no training in Lifestyle Medicine in the most recent 2 years.<span><sup>7</sup></span> Other surveys have revealed major gaps in nutrition teaching for medics with one survey finding only 45% of respondents had received any training on nutrition and generally low levels of self-confidence in managing nutrition-related issues.<span><sup>8</sup></span> Previous surveys among medical students have found low levels of basic knowledge about smoking, due to lack of training in how to address this.<span><sup>9, 10</sup></span></p><p>Turning to the concept of the double dividend, the same knowledge and skillset that underpins clinical competence is highly relevant and applicable to self-care and burnout prevention among medical students and healthcare professionals more broadly. The growing burden of anxiety, stress and other mental health disorders are increasingly challenging to manage among medical educators, trainers and medical managers.<span><sup>11</sup></span> Lifestyle Medicine teaching is therefore a preventive intervention for workforce well-being too. At Imperial College London, students today describe their negative health behaviours as ‘not very LMAP’ demonstrating how their clinical learning is potentially influencing their own health behaviour.</p><p>For more senior clinicians fearing that teaching well-being and positive health behaviours to medical students may be patronising, such anxieties can be allayed. While Lifestyle Medicine is currently delivered at postgraduate level through the International Board of Lifestyle Medicine Certification (Figure 1), the younger generation is more in touch and non-stigmatising in how it deals and relates to concepts of well-being and mental health. Seventy-six percent of U.K. students responding to a 2018 survey wanted Lifestyle Medicine to be incorporated into the curriculum at their medical school.<span><sup>7</sup></span> The recent growth in student-driven UK Lifestyle Medicine societies (supported by BSLM) is evidence that the younger generation recognises the value the specialty can provide. Regional conferences, such as the undergraduate Lifestyle Medicine Festival of the North in February 2022, have been warmly received by students.</p><p>Lifestyle Medicine teaching is about values, skills and knowledge (Figure 1). Memorising guidelines is insufficient if the skills to apply such understanding through motivational interviewing or coaching are not similarly developed. Instilling self-efficacy and confidence to deliver Lifestyle Medicine interventions as part of the clinical consultation offers great return on investment. The skills developed in Lifestyle Medicine are broad based, scalable and relevant to most, if not all clinical interactions.</p><p>We believe Lifestyle Medicine approaches are welcomed by patients too, although the literature in this area is comparatively less developed at present. Lifestyle Medicine is usually positioned within a frame of self-efficacy drawing on ideas of shared decision-making, personalised care and self-management. The centrality of relationships and the family unit is critical: both recognising family members as enablers of lifestyle change but also potential beneficiaries when diet or addictions are addressed. Similar to the benefits that lifestyle change can provide for healthcare providers, there are opportunities for similar gains among formal and informal carers too.</p><p>The public at large, driven by patient ambassadors (such as author AJ), is the key partner in articulating the Lifestyle Medicine argument. Lay proponents are central to pre-empting cynicism that suggests addressing lifestyle translates to blame and precedes the wholesale transfer of health responsibilities to patients. Lifestyle Medicine must not become an either–or. Instead, it is a starting point, a means of sustaining and augmenting more traditional medical approaches.</p><p>Embedding Lifestyle Medicine into the skillset of all our future doctors and clinicians is an opportunity to create a virtuous cycle that improves the health of our patients and our populations and protects our workforce ahead of a challenging and uncertain future. This can assist the public health workforce in their efforts to address wider determinants of health in a range of organisations. We contend Lifestyle Medicine must become a core component of undergraduate and postgraduate medical curricula.</p><p>Editor-in-Chief Fraser Birrell is also one of the authors.</p>\",\"PeriodicalId\":74076,\"journal\":{\"name\":\"Lifestyle medicine (Hoboken, N.J.)\",\"volume\":\"3 2\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-04-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/lim2.59\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Lifestyle medicine (Hoboken, N.J.)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/lim2.59\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Lifestyle medicine (Hoboken, N.J.)","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/lim2.59","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Is it time to embed Lifestyle Medicine in undergraduate and postgraduate curricula?
Some light at the end of the COVID-19 tunnel may be nearing. Yet, that same light is revealing a larger and longer term burden on our communities. Our educational institutions and health services have not been spared. The pandemic has catalysed the longer standing impact of anxiety, stress and burnout for many frontline health workers and younger people in particular. It has magnified socioeconomic and wider inequalities that are so detrimental to health and well-being.
While fiscal responses to the pandemic continue to be debated, there remains a fundamental barrier for the triad of Public Health, Social Care and Health Care resourcing: workforce. The historical absence of strategic workforce planning in the United Kingdom's National Health Services means that without extending (ethically challenging) international recruitment efforts, even substantial injections of finance into health and care economies are stymied by how such monies can be spent.
Lifestyle Medicine stands ready to yield a double dividend. First: to leverage self-care and health improvement amid the plethora of contact points that our communities have with public and third sector services. And second: to protect the health of our current and future workforce. While Lifestyle Medicine is no substitute for traditional population-level public health interventions, Lifestyle Medicine is an important and scalable element of the population health armamentarium, not least as systems seek increasingly integrated and preventive approaches to health and well-being. Behaviour change in the form of physical activity has been recently highlighted as a first-line therapy by U.K. health regulators in the management of depression (National Institute for Health and Care Excellent)2 and many other chronic physical health conditions. The relevance of health behaviours to mitigate communicable disease threats such as the COVID-19 pandemic will be clear in the minds of many. The need for skills in promoting lifestyle changes is endorsed as a core component of U.K. medical training.3
The specialty of Lifestyle Medicine, often described as emerging, can increasingly be described as maturing. As the American College of Lifestyle Medicine (ACLM) approaches 18 years of age, and the British Society of Lifestyle Medicine (BSLM) enters its seventh year, the global governance of the movement is transitioning too, with a new World Lifestyle Medicine Council. At the same time, consensus is being achieved on the specialty's scope: six pillars of lifestyle and increasingly concrete clinical application such as coaching, behaviour change and group consultations.
The evolution of interdisciplinary areas of practice is dependent on consensus - followed by convergence of both scope and practice. And while initially that involves interdisciplinary working, the extent to which Lifestyle Medicine is a logical expansion of scope for general practitioners or hospitalists versus a core multidisciplinary set of competencies is yet to be determined. While these two approaches are by no means mutually exclusive, we propose the former is desirable and the latter is essential. For the discipline to flourish, we need to integrate explicit Lifestyle Medicine competencies in a spiral approach throughout undergraduate and postgraduate training, with additional options to specialise and develop for those in senior posts looking to extend their practice.
In the United Kingdom, the (International Board) Certification in Lifestyle Medicine is the BSLM's first foray into the postgraduate space with non-medically qualified clinicians currently achieving the qualification alongside doctors. In parallel, work is also underway to establish Lifestyle Medicine in undergraduate curricula. At the front of this charge has been the innovative Lifestyle Medicine and Prevention (LMAP) modules that now form 15% of the core first 2 years of the Imperial College School of Medicine (ICSM) curriculum.
At Imperial, the Lifestyle Medicine agenda has proven an effective vehicle for Public Health to be taught through a more clinically oriented lens. The 1968 Todd Report on medical education cited Social Medicine (a predecessor to Public Health in medical curricula) as being ‘dull, neither useful nor difficult’. Few senior clinicians recall memories, and even fewer positive ones, of their own experience of Public Health during medical school.
Population Health is a broader term including public health medicine and wider disciplines (including non-medical interventions) that describes the amount of health and its distribution across a population.4 At the same time, the term Lifestyle Medicine has itself been criticised for diminishing the role that structural inequalities play in determining health outcomes, not least for socioeconomically disadvantaged groups.5 We argue the reverse is true. The teaching of Lifestyle Medicine (as a clinical approach) in the context of the wider determinants of health and associated inequalities (at population-level) is an avenue that can engender empathy and contextual understanding of patients’ decision-making and agency within clinical practice. Qualitative findings from two years of teaching with medical students at Imperial are already highlighting the understanding that a Lifestyle Medicine approach can establish. One student recently told us: ‘Initially it was very hard to understand why some people do particular things which can lead to a detriment to their health, but this module has helped me think in their shoes, which is essential if you want to… change… behaviour’.
The teaching of Lifestyle Medicine skills confers benefits for both future clinicians and the cadre of clinical teachers providing such training. Knowledge (or lack thereof) of health behaviours, guidelines and behaviour change among clinicians is cited as a reason that such initiatives are not offered in clinical consultations.6
Establishing clinician knowledge on evidence-based targets for physical activity, smoking cessation, alcohol consumption, sleep or healthy eating can too easily be put into the ‘common sense’ category and disregarded amid fierce competition for curriculum space during training. Eighty percent of U.K. medical students responding to a questionnaire in 2019 (N = 158) reported receiving no training in Lifestyle Medicine in the most recent 2 years.7 Other surveys have revealed major gaps in nutrition teaching for medics with one survey finding only 45% of respondents had received any training on nutrition and generally low levels of self-confidence in managing nutrition-related issues.8 Previous surveys among medical students have found low levels of basic knowledge about smoking, due to lack of training in how to address this.9, 10
Turning to the concept of the double dividend, the same knowledge and skillset that underpins clinical competence is highly relevant and applicable to self-care and burnout prevention among medical students and healthcare professionals more broadly. The growing burden of anxiety, stress and other mental health disorders are increasingly challenging to manage among medical educators, trainers and medical managers.11 Lifestyle Medicine teaching is therefore a preventive intervention for workforce well-being too. At Imperial College London, students today describe their negative health behaviours as ‘not very LMAP’ demonstrating how their clinical learning is potentially influencing their own health behaviour.
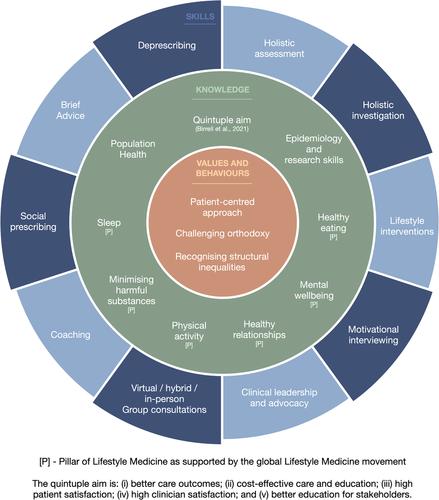
For more senior clinicians fearing that teaching well-being and positive health behaviours to medical students may be patronising, such anxieties can be allayed. While Lifestyle Medicine is currently delivered at postgraduate level through the International Board of Lifestyle Medicine Certification (Figure 1), the younger generation is more in touch and non-stigmatising in how it deals and relates to concepts of well-being and mental health. Seventy-six percent of U.K. students responding to a 2018 survey wanted Lifestyle Medicine to be incorporated into the curriculum at their medical school.7 The recent growth in student-driven UK Lifestyle Medicine societies (supported by BSLM) is evidence that the younger generation recognises the value the specialty can provide. Regional conferences, such as the undergraduate Lifestyle Medicine Festival of the North in February 2022, have been warmly received by students.
Lifestyle Medicine teaching is about values, skills and knowledge (Figure 1). Memorising guidelines is insufficient if the skills to apply such understanding through motivational interviewing or coaching are not similarly developed. Instilling self-efficacy and confidence to deliver Lifestyle Medicine interventions as part of the clinical consultation offers great return on investment. The skills developed in Lifestyle Medicine are broad based, scalable and relevant to most, if not all clinical interactions.
We believe Lifestyle Medicine approaches are welcomed by patients too, although the literature in this area is comparatively less developed at present. Lifestyle Medicine is usually positioned within a frame of self-efficacy drawing on ideas of shared decision-making, personalised care and self-management. The centrality of relationships and the family unit is critical: both recognising family members as enablers of lifestyle change but also potential beneficiaries when diet or addictions are addressed. Similar to the benefits that lifestyle change can provide for healthcare providers, there are opportunities for similar gains among formal and informal carers too.
The public at large, driven by patient ambassadors (such as author AJ), is the key partner in articulating the Lifestyle Medicine argument. Lay proponents are central to pre-empting cynicism that suggests addressing lifestyle translates to blame and precedes the wholesale transfer of health responsibilities to patients. Lifestyle Medicine must not become an either–or. Instead, it is a starting point, a means of sustaining and augmenting more traditional medical approaches.
Embedding Lifestyle Medicine into the skillset of all our future doctors and clinicians is an opportunity to create a virtuous cycle that improves the health of our patients and our populations and protects our workforce ahead of a challenging and uncertain future. This can assist the public health workforce in their efforts to address wider determinants of health in a range of organisations. We contend Lifestyle Medicine must become a core component of undergraduate and postgraduate medical curricula.
Editor-in-Chief Fraser Birrell is also one of the authors.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
