Fatemeh Mohammadpour Touserkani, Theodora Andriotis, Yaoping Zhang, Steven Pavlakis
{"title":"脑静脉血栓形成与B12缺乏","authors":"Fatemeh Mohammadpour Touserkani, Theodora Andriotis, Yaoping Zhang, Steven Pavlakis","doi":"10.1002/cns3.9","DOIUrl":null,"url":null,"abstract":"<p>Infants with prematurity and necrotizing enterocolitis (NEC) are at increased risk for short bowel syndrome and subsequent nutritional deficiencies. In particular, ileal resection is associated with vitamin B<sub>12</sub> malabsorption, which interferes with normal myelination and homocysteine metabolism.<span><sup>1, 2</sup></span> Vitamin B<sub>12</sub> deficiency is associated with neurodevelopmental delay as well as hyperhomocysteinemia, which increases the risk for venous thrombosis.<span><sup>2, 3</sup></span></p><p>This eight-year-old boy presented with severe headache, dehydration, and lethargy. He developed acute onset severe frontal headache followed by decreased oral intake, decreased urine output, and recurrent vomiting. The headache was dull and radiating to the back of his head. At the same time, he appeared to be sleepy and less active. These symptoms lasted for two to three days before he was brought to the primary doctor's office and then referred to the emergency department. On assessment, he was tired-looking and exhibited mild microcephaly, but his neurological examination was normal, as was an examination by an ophthalmologist.</p><p>He experienced mild global developmental delay. He was born at 25 weeks gestational age and had a prolonged stay in the neonatal intensive care unit, complicated by NEC and a hemicolectomy with ileostomy and removal of ileocecal valve. He had low normal levels of B<sub>12</sub> for several years prior to presentation and was not treated (151 pg/ml after surgery [normal 160-950]).</p><p>Brain magnetic resonance imaging and magnetic resonance venography (MRV) showed filling defects in the inferior sagittal, straight, torcula, and proximal transverse sinuses consistent with cerebral venous sinus thrombosis (CVST) with no evidence of acute infarction (Figure 1). Dehydration was initially considered to be the cause. Enoxaparin sodium was started at 1 mg/kg every 12 h with the goal of anti-Xa level between 0.5 and 1.0 U/ml. The hypercoagulation evaluation was normal. The B<sub>12</sub> level was 86 pg/ml. His hematocrit was 33.3, and his mean corpuscular volume (MCV) was 87.4. He was not treated at that time. He was discharged within a week after the repeat imaging remained stable with the goal to continue enoxaparin sodium for three months.</p><p>After three months, he again developed headache and lethargy, and MRV showed a new thrombus. Enoxaparin was switched to warfarin. After a year of warfarin, the clot resolved but he still had headaches. Two B<sub>12</sub> levels were obtained, both below 200. His anemia worsened (hematocrit 24.7) and his MCV increased to 96.9. The homocysteine level was 184 μmol/L (normal <11.4). At this point, he began B<sub>12</sub> injections (1000 mcg daily for one week followed by monthly and then quarterly injections thereafter). His B<sub>12</sub> levels normalized and remained normal throughout his course. The warfarin was discontinued and thrombus has not recurred.</p><p>Our patient had a difficult-to-treat CVST secondary to a condition predisposing to nutritional deficiency. His chronic B<sub>12</sub> deficiency was overlooked by his treating physicians until he presented with a profound deficiency with megaloblastic anemia.</p><p>The association between B<sub>12</sub> deficiency and CVST has been described in children with nutritional deficiency and megaloblastic anemia.<span><sup>4</sup></span> Previous authors suggested that testing for hyperhomocysteinemia and with B<sub>12</sub> supplementation should be considered in pediatric patients with CVST.<span><sup>5</sup></span> The diagnosis becomes even more crucial in patients with conditions known that promote nutritional deficiencies, such as a history of NEC and ileal surgery. In such children, early recognition of vitamin B<sub>12</sub> deficiency and timely vitamin supplementation may prevent the occurrence of CVST as well as other manifestations of B<sub>12</sub> deficiency, such as developmental delay.<span><sup>6, 7</sup></span> In this patient, the B<sub>12</sub> deficiency was chronic. While it is difficult to prove that the deficiency caused the CVST, it likley played a substantial role.</p><p>Hyperhomocysteinemia can damage the vascular endothelium, predisposing to thrombus formation.<span><sup>8, 9</sup></span> Consequently, vitamin B<sub>12</sub> deficiency is a potential risk factor in children with CVST.</p><p><b>Fatemeh Mohammadpour Touserkani</b>: Conceptualization; supervision; writing – original draft; writing – review and editing. <b>Theodora Andriotis</b>: Conceptualization; investigation; writing – original draft; writing – review and editing. <b>Yaoping Zhang</b>: Conceptualization; supervision; writing – original draft; writing – review and editing. <b>Steven Pavlakis</b>: Conceptualization; supervision; writing – original draft; writing – review and editing.</p><p>The authors declare no conflict of interest.</p>","PeriodicalId":72232,"journal":{"name":"Annals of the Child Neurology Society","volume":"1 2","pages":"152-154"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cns3.9","citationCount":"0","resultStr":"{\"title\":\"Cerebral venous thrombosis and B12 deficiency\",\"authors\":\"Fatemeh Mohammadpour Touserkani, Theodora Andriotis, Yaoping Zhang, Steven Pavlakis\",\"doi\":\"10.1002/cns3.9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Infants with prematurity and necrotizing enterocolitis (NEC) are at increased risk for short bowel syndrome and subsequent nutritional deficiencies. In particular, ileal resection is associated with vitamin B<sub>12</sub> malabsorption, which interferes with normal myelination and homocysteine metabolism.<span><sup>1, 2</sup></span> Vitamin B<sub>12</sub> deficiency is associated with neurodevelopmental delay as well as hyperhomocysteinemia, which increases the risk for venous thrombosis.<span><sup>2, 3</sup></span></p><p>This eight-year-old boy presented with severe headache, dehydration, and lethargy. He developed acute onset severe frontal headache followed by decreased oral intake, decreased urine output, and recurrent vomiting. The headache was dull and radiating to the back of his head. At the same time, he appeared to be sleepy and less active. These symptoms lasted for two to three days before he was brought to the primary doctor's office and then referred to the emergency department. On assessment, he was tired-looking and exhibited mild microcephaly, but his neurological examination was normal, as was an examination by an ophthalmologist.</p><p>He experienced mild global developmental delay. He was born at 25 weeks gestational age and had a prolonged stay in the neonatal intensive care unit, complicated by NEC and a hemicolectomy with ileostomy and removal of ileocecal valve. He had low normal levels of B<sub>12</sub> for several years prior to presentation and was not treated (151 pg/ml after surgery [normal 160-950]).</p><p>Brain magnetic resonance imaging and magnetic resonance venography (MRV) showed filling defects in the inferior sagittal, straight, torcula, and proximal transverse sinuses consistent with cerebral venous sinus thrombosis (CVST) with no evidence of acute infarction (Figure 1). Dehydration was initially considered to be the cause. Enoxaparin sodium was started at 1 mg/kg every 12 h with the goal of anti-Xa level between 0.5 and 1.0 U/ml. The hypercoagulation evaluation was normal. The B<sub>12</sub> level was 86 pg/ml. His hematocrit was 33.3, and his mean corpuscular volume (MCV) was 87.4. He was not treated at that time. He was discharged within a week after the repeat imaging remained stable with the goal to continue enoxaparin sodium for three months.</p><p>After three months, he again developed headache and lethargy, and MRV showed a new thrombus. Enoxaparin was switched to warfarin. After a year of warfarin, the clot resolved but he still had headaches. Two B<sub>12</sub> levels were obtained, both below 200. His anemia worsened (hematocrit 24.7) and his MCV increased to 96.9. The homocysteine level was 184 μmol/L (normal <11.4). At this point, he began B<sub>12</sub> injections (1000 mcg daily for one week followed by monthly and then quarterly injections thereafter). His B<sub>12</sub> levels normalized and remained normal throughout his course. The warfarin was discontinued and thrombus has not recurred.</p><p>Our patient had a difficult-to-treat CVST secondary to a condition predisposing to nutritional deficiency. His chronic B<sub>12</sub> deficiency was overlooked by his treating physicians until he presented with a profound deficiency with megaloblastic anemia.</p><p>The association between B<sub>12</sub> deficiency and CVST has been described in children with nutritional deficiency and megaloblastic anemia.<span><sup>4</sup></span> Previous authors suggested that testing for hyperhomocysteinemia and with B<sub>12</sub> supplementation should be considered in pediatric patients with CVST.<span><sup>5</sup></span> The diagnosis becomes even more crucial in patients with conditions known that promote nutritional deficiencies, such as a history of NEC and ileal surgery. In such children, early recognition of vitamin B<sub>12</sub> deficiency and timely vitamin supplementation may prevent the occurrence of CVST as well as other manifestations of B<sub>12</sub> deficiency, such as developmental delay.<span><sup>6, 7</sup></span> In this patient, the B<sub>12</sub> deficiency was chronic. While it is difficult to prove that the deficiency caused the CVST, it likley played a substantial role.</p><p>Hyperhomocysteinemia can damage the vascular endothelium, predisposing to thrombus formation.<span><sup>8, 9</sup></span> Consequently, vitamin B<sub>12</sub> deficiency is a potential risk factor in children with CVST.</p><p><b>Fatemeh Mohammadpour Touserkani</b>: Conceptualization; supervision; writing – original draft; writing – review and editing. <b>Theodora Andriotis</b>: Conceptualization; investigation; writing – original draft; writing – review and editing. <b>Yaoping Zhang</b>: Conceptualization; supervision; writing – original draft; writing – review and editing. <b>Steven Pavlakis</b>: Conceptualization; supervision; writing – original draft; writing – review and editing.</p><p>The authors declare no conflict of interest.</p>\",\"PeriodicalId\":72232,\"journal\":{\"name\":\"Annals of the Child Neurology Society\",\"volume\":\"1 2\",\"pages\":\"152-154\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cns3.9\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of the Child Neurology Society\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cns3.9\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of the Child Neurology Society","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cns3.9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Infants with prematurity and necrotizing enterocolitis (NEC) are at increased risk for short bowel syndrome and subsequent nutritional deficiencies. In particular, ileal resection is associated with vitamin B12 malabsorption, which interferes with normal myelination and homocysteine metabolism.1, 2 Vitamin B12 deficiency is associated with neurodevelopmental delay as well as hyperhomocysteinemia, which increases the risk for venous thrombosis.2, 3
This eight-year-old boy presented with severe headache, dehydration, and lethargy. He developed acute onset severe frontal headache followed by decreased oral intake, decreased urine output, and recurrent vomiting. The headache was dull and radiating to the back of his head. At the same time, he appeared to be sleepy and less active. These symptoms lasted for two to three days before he was brought to the primary doctor's office and then referred to the emergency department. On assessment, he was tired-looking and exhibited mild microcephaly, but his neurological examination was normal, as was an examination by an ophthalmologist.
He experienced mild global developmental delay. He was born at 25 weeks gestational age and had a prolonged stay in the neonatal intensive care unit, complicated by NEC and a hemicolectomy with ileostomy and removal of ileocecal valve. He had low normal levels of B12 for several years prior to presentation and was not treated (151 pg/ml after surgery [normal 160-950]).
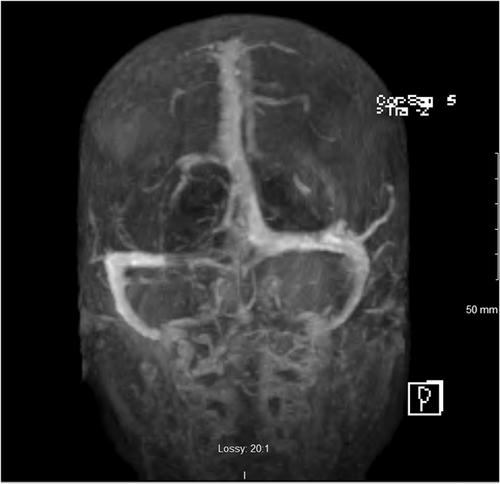
Brain magnetic resonance imaging and magnetic resonance venography (MRV) showed filling defects in the inferior sagittal, straight, torcula, and proximal transverse sinuses consistent with cerebral venous sinus thrombosis (CVST) with no evidence of acute infarction (Figure 1). Dehydration was initially considered to be the cause. Enoxaparin sodium was started at 1 mg/kg every 12 h with the goal of anti-Xa level between 0.5 and 1.0 U/ml. The hypercoagulation evaluation was normal. The B12 level was 86 pg/ml. His hematocrit was 33.3, and his mean corpuscular volume (MCV) was 87.4. He was not treated at that time. He was discharged within a week after the repeat imaging remained stable with the goal to continue enoxaparin sodium for three months.
After three months, he again developed headache and lethargy, and MRV showed a new thrombus. Enoxaparin was switched to warfarin. After a year of warfarin, the clot resolved but he still had headaches. Two B12 levels were obtained, both below 200. His anemia worsened (hematocrit 24.7) and his MCV increased to 96.9. The homocysteine level was 184 μmol/L (normal <11.4). At this point, he began B12 injections (1000 mcg daily for one week followed by monthly and then quarterly injections thereafter). His B12 levels normalized and remained normal throughout his course. The warfarin was discontinued and thrombus has not recurred.
Our patient had a difficult-to-treat CVST secondary to a condition predisposing to nutritional deficiency. His chronic B12 deficiency was overlooked by his treating physicians until he presented with a profound deficiency with megaloblastic anemia.
The association between B12 deficiency and CVST has been described in children with nutritional deficiency and megaloblastic anemia.4 Previous authors suggested that testing for hyperhomocysteinemia and with B12 supplementation should be considered in pediatric patients with CVST.5 The diagnosis becomes even more crucial in patients with conditions known that promote nutritional deficiencies, such as a history of NEC and ileal surgery. In such children, early recognition of vitamin B12 deficiency and timely vitamin supplementation may prevent the occurrence of CVST as well as other manifestations of B12 deficiency, such as developmental delay.6, 7 In this patient, the B12 deficiency was chronic. While it is difficult to prove that the deficiency caused the CVST, it likley played a substantial role.
Hyperhomocysteinemia can damage the vascular endothelium, predisposing to thrombus formation.8, 9 Consequently, vitamin B12 deficiency is a potential risk factor in children with CVST.
Fatemeh Mohammadpour Touserkani: Conceptualization; supervision; writing – original draft; writing – review and editing. Theodora Andriotis: Conceptualization; investigation; writing – original draft; writing – review and editing. Yaoping Zhang: Conceptualization; supervision; writing – original draft; writing – review and editing. Steven Pavlakis: Conceptualization; supervision; writing – original draft; writing – review and editing.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
