Joshua K. Kays MD, Tiffany W. Liang MD, Teresa A. Zimmers PhD, Daniel P. Milgrom MD, Hamzah Abduljabar BS, Andrew Young BS, Bradford J. Kim MD MHS, Teresa M. Bell PhD, Andres Fajardo MD, Michael P. Murphy MD, Leonidas G. Koniaris MD MBA
{"title":"肌少症是腹主动脉瘤修复后死亡率的重要预测因子","authors":"Joshua K. Kays MD, Tiffany W. Liang MD, Teresa A. Zimmers PhD, Daniel P. Milgrom MD, Hamzah Abduljabar BS, Andrew Young BS, Bradford J. Kim MD MHS, Teresa M. Bell PhD, Andres Fajardo MD, Michael P. Murphy MD, Leonidas G. Koniaris MD MBA","doi":"10.17987/jcsm-cr.v3i1.53","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aims</h3>\n \n <p>Repair of abdominal aortic aneurysms (AAA) decreases the incidence of rupture and death. In cancer patients, sarcopenia has been associated with increased surgical complications and mortality. The impact of sarcopenia on survival after AAA repair has yet to be described.</p>\n </section>\n \n <section>\n \n <h3> Methods and Results</h3>\n \n <p>Patient demographic, laboratory, body composition measurements and survival data were obtained from patients undergoing AAA repair at the Indiana University medical campus over a 5-year period. Univariate and multivariate analyses were performed to identify factors associated with overall survival. Overall, 58.2% presented with sarcopenia. Sarcopenic patients were older (71.8±8.3 versus 66.8±8.1 years; p<0.001), had lower body mass index (BMI) (26.3±5.2 versus 31.5±5.9 kg/m<sup>2</sup>; p<0.001), higher rates of myosteatosis (84.4% versus 52.%; p<0.001), greater AAA diameter (60.6±14.0 versus 57.8±11.7 mm; p=0.016), higher Charlson Comorbidity Index (CCI) (32.3% versus 25.1% ≥6; p=0.034), and increased rates of rupture (8.2% versus 3.8%; p=0.047). Sarcopenic and nonsarcopenic patients had no difference in 30-day morbidity (8.5% versus 8.5%; p=0.991) or mortality (3.7% versus 0.9%; p=0.07). Univariate analysis demonstrated age, sarcopenia, myosteatosis, CCI, and BMI to be associated with long-term survival. There was no correlation between BMI and sarcopenia. Both sarcopenia and myosteatosis resulted in decreased one-, three-, and five-year survivals compared to their counterparts. On multivariate analysis sarcopenia is independently associated with survival, conferring a 1.6-fold increase in death (p=0.04). The combination of sarcopenia plus myosteatosis doubled the risk of death compared to sarcopenia alone.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>This is the first study to demonstrate that over half of all patients undergoing AAA repair are sarcopenic, a condition associated with increased mortality. Sarcopenia with myosteatosis is associated with double the mortality of sarcopenia alone. CT scan, but not BMI, accurately identifies sarcopenia and myosteatosis. Defining the mechanisms through which sarcopenia contributes to late death after AAA repair is critical to developing novel interventions that may improve survival in this high risk population.</p>\n </section>\n </div>","PeriodicalId":73543,"journal":{"name":"JCSM clinical reports","volume":"3 1","pages":"1-12"},"PeriodicalIF":0.0000,"publicationDate":"2018-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.17987/jcsm-cr.v3i1.53","citationCount":"18","resultStr":"{\"title\":\"Sarcopenia is a Significant Predictor of Mortality After Abdominal Aortic Aneurysm Repair\",\"authors\":\"Joshua K. Kays MD, Tiffany W. Liang MD, Teresa A. Zimmers PhD, Daniel P. Milgrom MD, Hamzah Abduljabar BS, Andrew Young BS, Bradford J. Kim MD MHS, Teresa M. Bell PhD, Andres Fajardo MD, Michael P. Murphy MD, Leonidas G. Koniaris MD MBA\",\"doi\":\"10.17987/jcsm-cr.v3i1.53\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aims</h3>\\n \\n <p>Repair of abdominal aortic aneurysms (AAA) decreases the incidence of rupture and death. In cancer patients, sarcopenia has been associated with increased surgical complications and mortality. The impact of sarcopenia on survival after AAA repair has yet to be described.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods and Results</h3>\\n \\n <p>Patient demographic, laboratory, body composition measurements and survival data were obtained from patients undergoing AAA repair at the Indiana University medical campus over a 5-year period. Univariate and multivariate analyses were performed to identify factors associated with overall survival. Overall, 58.2% presented with sarcopenia. Sarcopenic patients were older (71.8±8.3 versus 66.8±8.1 years; p<0.001), had lower body mass index (BMI) (26.3±5.2 versus 31.5±5.9 kg/m<sup>2</sup>; p<0.001), higher rates of myosteatosis (84.4% versus 52.%; p<0.001), greater AAA diameter (60.6±14.0 versus 57.8±11.7 mm; p=0.016), higher Charlson Comorbidity Index (CCI) (32.3% versus 25.1% ≥6; p=0.034), and increased rates of rupture (8.2% versus 3.8%; p=0.047). Sarcopenic and nonsarcopenic patients had no difference in 30-day morbidity (8.5% versus 8.5%; p=0.991) or mortality (3.7% versus 0.9%; p=0.07). Univariate analysis demonstrated age, sarcopenia, myosteatosis, CCI, and BMI to be associated with long-term survival. There was no correlation between BMI and sarcopenia. Both sarcopenia and myosteatosis resulted in decreased one-, three-, and five-year survivals compared to their counterparts. On multivariate analysis sarcopenia is independently associated with survival, conferring a 1.6-fold increase in death (p=0.04). The combination of sarcopenia plus myosteatosis doubled the risk of death compared to sarcopenia alone.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>This is the first study to demonstrate that over half of all patients undergoing AAA repair are sarcopenic, a condition associated with increased mortality. Sarcopenia with myosteatosis is associated with double the mortality of sarcopenia alone. CT scan, but not BMI, accurately identifies sarcopenia and myosteatosis. Defining the mechanisms through which sarcopenia contributes to late death after AAA repair is critical to developing novel interventions that may improve survival in this high risk population.</p>\\n </section>\\n </div>\",\"PeriodicalId\":73543,\"journal\":{\"name\":\"JCSM clinical reports\",\"volume\":\"3 1\",\"pages\":\"1-12\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2018-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.17987/jcsm-cr.v3i1.53\",\"citationCount\":\"18\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JCSM clinical reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.17987/jcsm-cr.v3i1.53\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCSM clinical reports","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.17987/jcsm-cr.v3i1.53","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 18
摘要
目的腹主动脉瘤修复术可降低其破裂和死亡的发生率。在癌症患者中,肌肉减少症与手术并发症和死亡率增加有关。肌少症对AAA修复后存活的影响尚未被描述。方法和结果在印第安纳大学医学院接受AAA修复的患者中获得了5年的患者人口统计学、实验室、身体成分测量和生存数据。进行单因素和多因素分析以确定与总生存率相关的因素。总体而言,58.2%表现为肌肉减少症。肌肉减少症患者年龄较大(71.8±8.3岁vs 66.8±8.1岁);p<0.001),体重指数(BMI)较低(26.3±5.2 vs 31.5±5.9 kg/m2;P<0.001),骨骼肌病的发病率更高(84.4%对52.2%;p<0.001),更大的AAA直径(60.6±14.0 vs 57.8±11.7 mm;p=0.016),较高的Charlson合并症指数(CCI) (32.3% vs 25.1%≥6;P =0.034),破裂率增加(8.2% vs 3.8%;p = 0.047)。肌肉减少症和非肌肉减少症患者的30天发病率无差异(8.5% vs 8.5%;P =0.991)或死亡率(3.7% vs 0.9%;p = 0.07)。单因素分析表明,年龄、肌肉减少症、肌骨化症、CCI和BMI与长期生存相关。BMI和肌肉减少症之间没有相关性。与同类患者相比,肌肉减少症和骨骼肌病的1年、3年和5年生存率均下降。在多变量分析中,肌肉减少症与生存率独立相关,死亡率增加1.6倍(p=0.04)。与单纯的肌肉减少症相比,肌肉减少症合并肌骨化症的死亡风险增加了一倍。这是首次有研究表明,接受AAA修复的患者中有一半以上是肌肉减少症,这种疾病与死亡率增加有关。肌少症合并骨骼肌病的死亡率是单纯肌少症的两倍。CT扫描,而不是BMI,可以准确地识别肌肉减少症和肌骨化症。明确肌少症导致AAA修复后晚期死亡的机制,对于开发新的干预措施,提高这一高危人群的生存率至关重要。
Sarcopenia is a Significant Predictor of Mortality After Abdominal Aortic Aneurysm Repair
Aims
Repair of abdominal aortic aneurysms (AAA) decreases the incidence of rupture and death. In cancer patients, sarcopenia has been associated with increased surgical complications and mortality. The impact of sarcopenia on survival after AAA repair has yet to be described.
Methods and Results
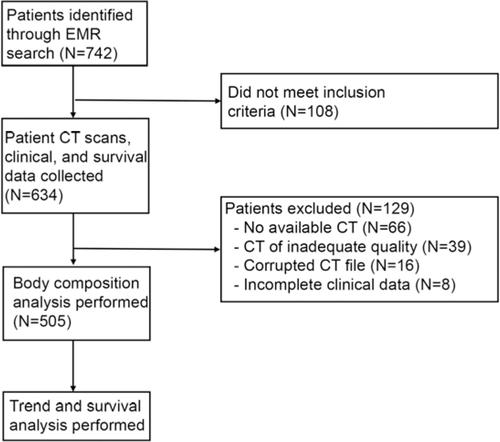
Patient demographic, laboratory, body composition measurements and survival data were obtained from patients undergoing AAA repair at the Indiana University medical campus over a 5-year period. Univariate and multivariate analyses were performed to identify factors associated with overall survival. Overall, 58.2% presented with sarcopenia. Sarcopenic patients were older (71.8±8.3 versus 66.8±8.1 years; p<0.001), had lower body mass index (BMI) (26.3±5.2 versus 31.5±5.9 kg/m2; p<0.001), higher rates of myosteatosis (84.4% versus 52.%; p<0.001), greater AAA diameter (60.6±14.0 versus 57.8±11.7 mm; p=0.016), higher Charlson Comorbidity Index (CCI) (32.3% versus 25.1% ≥6; p=0.034), and increased rates of rupture (8.2% versus 3.8%; p=0.047). Sarcopenic and nonsarcopenic patients had no difference in 30-day morbidity (8.5% versus 8.5%; p=0.991) or mortality (3.7% versus 0.9%; p=0.07). Univariate analysis demonstrated age, sarcopenia, myosteatosis, CCI, and BMI to be associated with long-term survival. There was no correlation between BMI and sarcopenia. Both sarcopenia and myosteatosis resulted in decreased one-, three-, and five-year survivals compared to their counterparts. On multivariate analysis sarcopenia is independently associated with survival, conferring a 1.6-fold increase in death (p=0.04). The combination of sarcopenia plus myosteatosis doubled the risk of death compared to sarcopenia alone.
Conclusions
This is the first study to demonstrate that over half of all patients undergoing AAA repair are sarcopenic, a condition associated with increased mortality. Sarcopenia with myosteatosis is associated with double the mortality of sarcopenia alone. CT scan, but not BMI, accurately identifies sarcopenia and myosteatosis. Defining the mechanisms through which sarcopenia contributes to late death after AAA repair is critical to developing novel interventions that may improve survival in this high risk population.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
