Mostafa Mohrag, Mohammed Abdulrasak, Mohammed Binsalman, Majid Darraj
{"title":"一例挑战性疾病的病例报告:免疫球蛋白G4相关疾病伴急性肾损伤。","authors":"Mostafa Mohrag, Mohammed Abdulrasak, Mohammed Binsalman, Majid Darraj","doi":"10.14740/jmc4159","DOIUrl":null,"url":null,"abstract":"<p><p>Immunoglobulin G4-related disease (IgG4-RD), which was initially identified as a type of autoimmune pancreatitis around the year 2000, is now widely acknowledged to be a systemic sickness. Based on both general and organ-specific criteria, alongside laboratory measurements of IgG4-subtype, the diagnosis is made. The diagnosis requires, however, a heightened index of suspicion, especially given the nonspecific clinical presentation. In addition to this, the symptoms may be \"disseminated\" in time and the multitude of organ-system involvement may seem initially unrelated. Furthermore, IgG4 levels may be falsely normal especially during the first presentation of IgG4-RD. We report a case of a 33-year-old male who was referred by his general practitioner (GP) to the fast access nephrology clinic due to elevated creatinine and fatigue, which was found after the patient had undergone some investigations at the GP office. He had history of atopic dermatitis and a prior admission for acute pancreatitis of unknown cause and recent bilateral anterior uveitis treated with steroid eyedrops. His urinalysis showed one to two granular casts per high-power field (HPF), and his creatinine was 262 µmol/L (previously normal). Three main differential diagnoses were considered given the patient's history: sarcoidosis, tubulointerstitial nephritis with uveitis (TINU) and IgG4-related disorder. Investigations were undertaken in that regard showing elevated serum IgG4 levels (2.7 times upper-limit of normal). Renal biopsy demonstrated tubulointerstitial nephritis (TIN) with 30 IgG4-positive plasma cells per HPF. Given the patient's presentation over time, a diagnosis of IgG4-TIN was considered. The patient was treated with high-dose steroids and has shown signs of improvement of both his renal and ocular problems. The uniqueness of the case is reflected through the fact that IgG4-renal disease is usually diagnosed in patients with an already established manifestation of another organ, whilst in our patient the renal involvement led to establishing IgG4-RD. It is also important to note that, in spite of initially negative serum IgG4 levels, the diagnosis still needs to be considered especially if multisystem involvement is present (as in this case).</p>","PeriodicalId":101328,"journal":{"name":"Journal of medical cases","volume":"14 9-10","pages":"339-343"},"PeriodicalIF":0.9000,"publicationDate":"2023-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3f/d5/jmc-14-339.PMC10586334.pdf","citationCount":"0","resultStr":"{\"title\":\"A Case Report of a Challenging Disease: Immunoglobulin G4-Related Disease With Acute Kideny Injury.\",\"authors\":\"Mostafa Mohrag, Mohammed Abdulrasak, Mohammed Binsalman, Majid Darraj\",\"doi\":\"10.14740/jmc4159\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Immunoglobulin G4-related disease (IgG4-RD), which was initially identified as a type of autoimmune pancreatitis around the year 2000, is now widely acknowledged to be a systemic sickness. Based on both general and organ-specific criteria, alongside laboratory measurements of IgG4-subtype, the diagnosis is made. The diagnosis requires, however, a heightened index of suspicion, especially given the nonspecific clinical presentation. In addition to this, the symptoms may be \\\"disseminated\\\" in time and the multitude of organ-system involvement may seem initially unrelated. Furthermore, IgG4 levels may be falsely normal especially during the first presentation of IgG4-RD. We report a case of a 33-year-old male who was referred by his general practitioner (GP) to the fast access nephrology clinic due to elevated creatinine and fatigue, which was found after the patient had undergone some investigations at the GP office. He had history of atopic dermatitis and a prior admission for acute pancreatitis of unknown cause and recent bilateral anterior uveitis treated with steroid eyedrops. His urinalysis showed one to two granular casts per high-power field (HPF), and his creatinine was 262 µmol/L (previously normal). Three main differential diagnoses were considered given the patient's history: sarcoidosis, tubulointerstitial nephritis with uveitis (TINU) and IgG4-related disorder. Investigations were undertaken in that regard showing elevated serum IgG4 levels (2.7 times upper-limit of normal). Renal biopsy demonstrated tubulointerstitial nephritis (TIN) with 30 IgG4-positive plasma cells per HPF. Given the patient's presentation over time, a diagnosis of IgG4-TIN was considered. The patient was treated with high-dose steroids and has shown signs of improvement of both his renal and ocular problems. The uniqueness of the case is reflected through the fact that IgG4-renal disease is usually diagnosed in patients with an already established manifestation of another organ, whilst in our patient the renal involvement led to establishing IgG4-RD. It is also important to note that, in spite of initially negative serum IgG4 levels, the diagnosis still needs to be considered especially if multisystem involvement is present (as in this case).</p>\",\"PeriodicalId\":101328,\"journal\":{\"name\":\"Journal of medical cases\",\"volume\":\"14 9-10\",\"pages\":\"339-343\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2023-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3f/d5/jmc-14-339.PMC10586334.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of medical cases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jmc4159\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/10/13 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of medical cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jmc4159","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/13 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
A Case Report of a Challenging Disease: Immunoglobulin G4-Related Disease With Acute Kideny Injury.
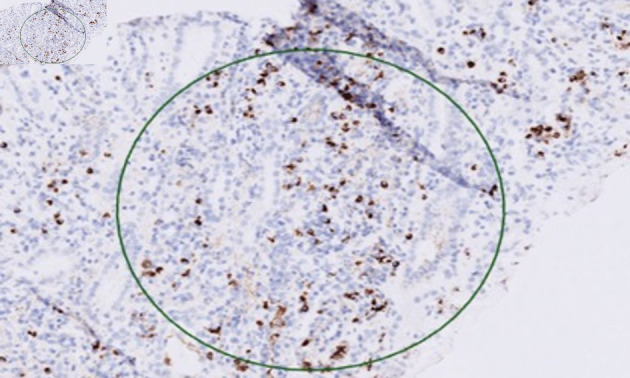
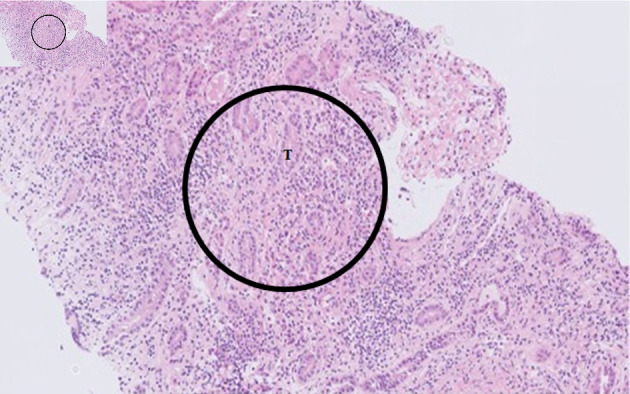
Immunoglobulin G4-related disease (IgG4-RD), which was initially identified as a type of autoimmune pancreatitis around the year 2000, is now widely acknowledged to be a systemic sickness. Based on both general and organ-specific criteria, alongside laboratory measurements of IgG4-subtype, the diagnosis is made. The diagnosis requires, however, a heightened index of suspicion, especially given the nonspecific clinical presentation. In addition to this, the symptoms may be "disseminated" in time and the multitude of organ-system involvement may seem initially unrelated. Furthermore, IgG4 levels may be falsely normal especially during the first presentation of IgG4-RD. We report a case of a 33-year-old male who was referred by his general practitioner (GP) to the fast access nephrology clinic due to elevated creatinine and fatigue, which was found after the patient had undergone some investigations at the GP office. He had history of atopic dermatitis and a prior admission for acute pancreatitis of unknown cause and recent bilateral anterior uveitis treated with steroid eyedrops. His urinalysis showed one to two granular casts per high-power field (HPF), and his creatinine was 262 µmol/L (previously normal). Three main differential diagnoses were considered given the patient's history: sarcoidosis, tubulointerstitial nephritis with uveitis (TINU) and IgG4-related disorder. Investigations were undertaken in that regard showing elevated serum IgG4 levels (2.7 times upper-limit of normal). Renal biopsy demonstrated tubulointerstitial nephritis (TIN) with 30 IgG4-positive plasma cells per HPF. Given the patient's presentation over time, a diagnosis of IgG4-TIN was considered. The patient was treated with high-dose steroids and has shown signs of improvement of both his renal and ocular problems. The uniqueness of the case is reflected through the fact that IgG4-renal disease is usually diagnosed in patients with an already established manifestation of another organ, whilst in our patient the renal involvement led to establishing IgG4-RD. It is also important to note that, in spite of initially negative serum IgG4 levels, the diagnosis still needs to be considered especially if multisystem involvement is present (as in this case).



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
