{"title":"模拟术后出血的脑肿瘤活检开颅术后自发性颅内低血压。","authors":"Joji Inamasu, Masashi Fujisawa, Mizuto Sato","doi":"10.2176/jns-nmc.2023-0139","DOIUrl":null,"url":null,"abstract":"<p><p>In this study, we report on a previously healthy 44-year-old man who underwent an open biopsy under general anesthesia for a tumorous lesion found in his left frontal lobe via a small supratentorial craniotomy. While both postoperative course and brain computed tomography (CT) scans had been considered unremarkable, the patient became stuporous on postoperative day (POD) 4. A brain CT obtained on that day showed a subdural hematoma with marked brain shift which we thought might have been due to postoperative bleeding; he was immediately brought to an operating theater for hematoma removal. However, no bleeding source was found, and the brain remained depressed after hematoma evacuation. Furthermore, the brain shift remained unchanged on postoperative CT. While spontaneous intracranial hypotension (SIH) was considered, imaging studies to search for possible cerebrospinal fluid (CSF) leakage in the spinal column were not performed as the patient's condition has improved. However, he became stuporous again on POD 8, which urged us to perform CT myelogram. The CT myelogram showed a massive CSF leakage at the L1-L2 level. Subsequent autologous blood patch has successfully terminated the CSF leakage, and he became fully oriented shortly after the blood patch therapy. Thus, it should be noted that SIH may occur during postoperative period of intracranial surgery, and it may manifest radiographically as a subdural hematoma indistinguishable from postoperative bleeding. SIH should also be included in a differential diagnosis of postoperative headache, regardless of its characteristics, because headache associated with SIH may not always be orthostatic.</p>","PeriodicalId":101331,"journal":{"name":"NMC case report journal","volume":"10 ","pages":"247-252"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0a/de/2188-4226-10-0247.PMC10584665.pdf","citationCount":"0","resultStr":"{\"title\":\"Spontaneous Intracranial Hypotension Occurring after Craniotomy for Brain Tumor Biopsy Mimicking Postoperative Bleeding.\",\"authors\":\"Joji Inamasu, Masashi Fujisawa, Mizuto Sato\",\"doi\":\"10.2176/jns-nmc.2023-0139\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>In this study, we report on a previously healthy 44-year-old man who underwent an open biopsy under general anesthesia for a tumorous lesion found in his left frontal lobe via a small supratentorial craniotomy. While both postoperative course and brain computed tomography (CT) scans had been considered unremarkable, the patient became stuporous on postoperative day (POD) 4. A brain CT obtained on that day showed a subdural hematoma with marked brain shift which we thought might have been due to postoperative bleeding; he was immediately brought to an operating theater for hematoma removal. However, no bleeding source was found, and the brain remained depressed after hematoma evacuation. Furthermore, the brain shift remained unchanged on postoperative CT. While spontaneous intracranial hypotension (SIH) was considered, imaging studies to search for possible cerebrospinal fluid (CSF) leakage in the spinal column were not performed as the patient's condition has improved. However, he became stuporous again on POD 8, which urged us to perform CT myelogram. The CT myelogram showed a massive CSF leakage at the L1-L2 level. Subsequent autologous blood patch has successfully terminated the CSF leakage, and he became fully oriented shortly after the blood patch therapy. Thus, it should be noted that SIH may occur during postoperative period of intracranial surgery, and it may manifest radiographically as a subdural hematoma indistinguishable from postoperative bleeding. SIH should also be included in a differential diagnosis of postoperative headache, regardless of its characteristics, because headache associated with SIH may not always be orthostatic.</p>\",\"PeriodicalId\":101331,\"journal\":{\"name\":\"NMC case report journal\",\"volume\":\"10 \",\"pages\":\"247-252\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-09-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0a/de/2188-4226-10-0247.PMC10584665.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"NMC case report journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2176/jns-nmc.2023-0139\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"NMC case report journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2176/jns-nmc.2023-0139","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Spontaneous Intracranial Hypotension Occurring after Craniotomy for Brain Tumor Biopsy Mimicking Postoperative Bleeding.
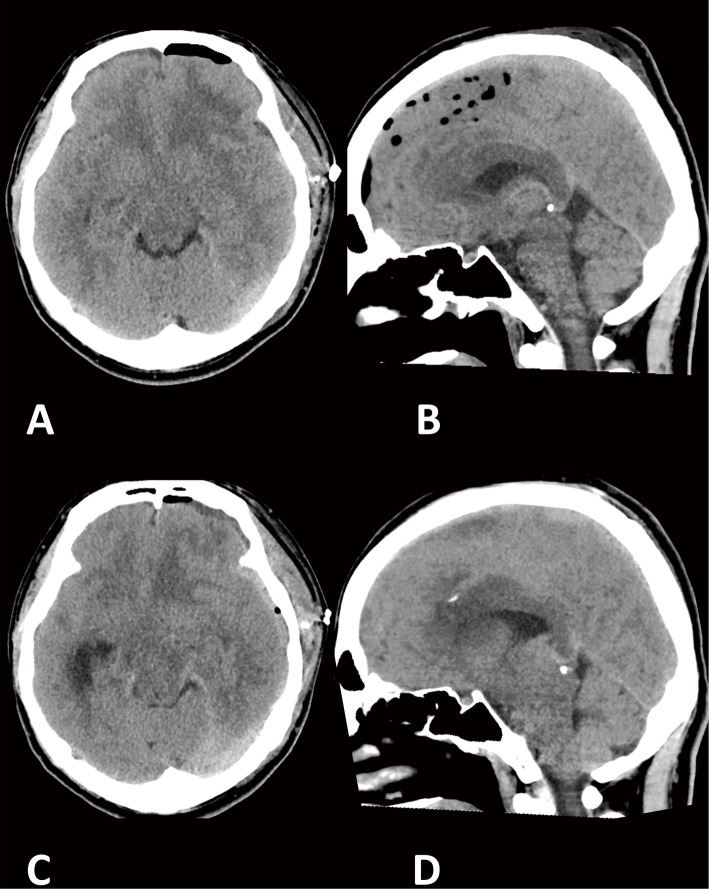
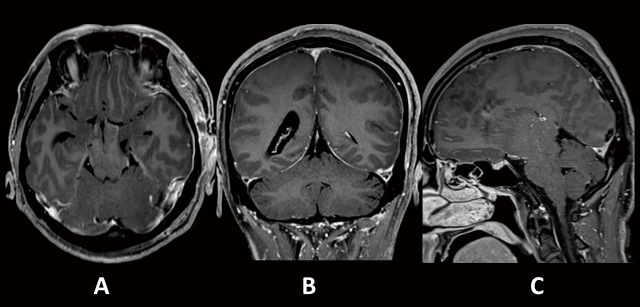
In this study, we report on a previously healthy 44-year-old man who underwent an open biopsy under general anesthesia for a tumorous lesion found in his left frontal lobe via a small supratentorial craniotomy. While both postoperative course and brain computed tomography (CT) scans had been considered unremarkable, the patient became stuporous on postoperative day (POD) 4. A brain CT obtained on that day showed a subdural hematoma with marked brain shift which we thought might have been due to postoperative bleeding; he was immediately brought to an operating theater for hematoma removal. However, no bleeding source was found, and the brain remained depressed after hematoma evacuation. Furthermore, the brain shift remained unchanged on postoperative CT. While spontaneous intracranial hypotension (SIH) was considered, imaging studies to search for possible cerebrospinal fluid (CSF) leakage in the spinal column were not performed as the patient's condition has improved. However, he became stuporous again on POD 8, which urged us to perform CT myelogram. The CT myelogram showed a massive CSF leakage at the L1-L2 level. Subsequent autologous blood patch has successfully terminated the CSF leakage, and he became fully oriented shortly after the blood patch therapy. Thus, it should be noted that SIH may occur during postoperative period of intracranial surgery, and it may manifest radiographically as a subdural hematoma indistinguishable from postoperative bleeding. SIH should also be included in a differential diagnosis of postoperative headache, regardless of its characteristics, because headache associated with SIH may not always be orthostatic.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
