Osama M Eldadah, Asseel Ali Alsalmi, Obayda M Diraneyya, Abdah A Hrfi, Mohammed H A Mohammed, Maria L Valls, Abdullah A Alghamdi
{"title":"主动脉缩窄修复后残余梯度的进行性变化及其在再干预预测中的作用:一项纵向数据分析。","authors":"Osama M Eldadah, Asseel Ali Alsalmi, Obayda M Diraneyya, Abdah A Hrfi, Mohammed H A Mohammed, Maria L Valls, Abdullah A Alghamdi","doi":"10.4103/apc.apc_140_22","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Repair of aortic coarctation through left thoracotomy is the standard treatment when anatomically feasible. Long-term outcomes are well studied, including the need for reintervention. However, the timely variation in residual gradients across the repaired segment is ill-defined. The aim of this work was to study the progressive changes of estimated peak gradient (ePG) acquired by transthoracic continuous-wave Doppler echocardiography across the aortic arch after repair and to assess the role of timing of assessment and values of ePG in prediction of reintervention.</p><p><strong>Materials and methods: </strong>All eligible patients for this study who underwent aortic coarctation repair through left thoracotomy from 2001 to 2017 were reviewed. Details of the aortic arch dimensions and associated lesions were obtained by transthoracic echocardiography (TTE). The primary outcome was the ePG across the aortic arch after repair. Longitudinal data analyses with mixed effect modeling were used to determine independent predictors for ePGs.</p><p><strong>Results: </strong>A total of 312 patients were included. Median age and weight were 30 days and 4 kg, respectively. Associated lesions included ventricular septal defect (VSD) (53%), bicuspid aortic valve (53%) and mitral stenosis (25%). Over 15-years follow-up the freedom from reintervention was 92.3%, while 24 out of the 312 patients underwent reintervention (7.7%). Longitudinal data analyses of serial 2566 TTE studies were done. The graphical display showed that the ePG across coarctation area in the first postoperative TTE was the most notable difference between those who underwent reintervention and those who did not. Further testing with proportional hazard and logistic regression modeling confirmed this finding. The area under receiver operating curve statistics showed that an ePG of 25 mmHg is an optimal cutoff value for the prediction of the reintervention.</p><p><strong>Conclusions: </strong>The ePG acquired in the first postoperative TTE is the most important predictor for reinterventions. The presence of VSD is associated with decreased ePGs. We propose that an ePG in the first postoperative TTE of 25 mmHg or more is a strong predictor for the need of reintervention.</p>","PeriodicalId":8026,"journal":{"name":"Annals of Pediatric Cardiology","volume":"16 3","pages":"182-188"},"PeriodicalIF":0.7000,"publicationDate":"2023-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ca/b6/APC-16-182.PMC10593279.pdf","citationCount":"0","resultStr":"{\"title\":\"Progressive changes in residual gradient after aortic coarctation repair and its role in the prediction of reintervention: A longitudinal data analysis.\",\"authors\":\"Osama M Eldadah, Asseel Ali Alsalmi, Obayda M Diraneyya, Abdah A Hrfi, Mohammed H A Mohammed, Maria L Valls, Abdullah A Alghamdi\",\"doi\":\"10.4103/apc.apc_140_22\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Repair of aortic coarctation through left thoracotomy is the standard treatment when anatomically feasible. Long-term outcomes are well studied, including the need for reintervention. However, the timely variation in residual gradients across the repaired segment is ill-defined. The aim of this work was to study the progressive changes of estimated peak gradient (ePG) acquired by transthoracic continuous-wave Doppler echocardiography across the aortic arch after repair and to assess the role of timing of assessment and values of ePG in prediction of reintervention.</p><p><strong>Materials and methods: </strong>All eligible patients for this study who underwent aortic coarctation repair through left thoracotomy from 2001 to 2017 were reviewed. Details of the aortic arch dimensions and associated lesions were obtained by transthoracic echocardiography (TTE). The primary outcome was the ePG across the aortic arch after repair. Longitudinal data analyses with mixed effect modeling were used to determine independent predictors for ePGs.</p><p><strong>Results: </strong>A total of 312 patients were included. Median age and weight were 30 days and 4 kg, respectively. Associated lesions included ventricular septal defect (VSD) (53%), bicuspid aortic valve (53%) and mitral stenosis (25%). Over 15-years follow-up the freedom from reintervention was 92.3%, while 24 out of the 312 patients underwent reintervention (7.7%). Longitudinal data analyses of serial 2566 TTE studies were done. The graphical display showed that the ePG across coarctation area in the first postoperative TTE was the most notable difference between those who underwent reintervention and those who did not. Further testing with proportional hazard and logistic regression modeling confirmed this finding. The area under receiver operating curve statistics showed that an ePG of 25 mmHg is an optimal cutoff value for the prediction of the reintervention.</p><p><strong>Conclusions: </strong>The ePG acquired in the first postoperative TTE is the most important predictor for reinterventions. The presence of VSD is associated with decreased ePGs. We propose that an ePG in the first postoperative TTE of 25 mmHg or more is a strong predictor for the need of reintervention.</p>\",\"PeriodicalId\":8026,\"journal\":{\"name\":\"Annals of Pediatric Cardiology\",\"volume\":\"16 3\",\"pages\":\"182-188\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2023-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ca/b6/APC-16-182.PMC10593279.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Pediatric Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/apc.apc_140_22\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/9/8 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Pediatric Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/apc.apc_140_22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/8 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Progressive changes in residual gradient after aortic coarctation repair and its role in the prediction of reintervention: A longitudinal data analysis.
Background: Repair of aortic coarctation through left thoracotomy is the standard treatment when anatomically feasible. Long-term outcomes are well studied, including the need for reintervention. However, the timely variation in residual gradients across the repaired segment is ill-defined. The aim of this work was to study the progressive changes of estimated peak gradient (ePG) acquired by transthoracic continuous-wave Doppler echocardiography across the aortic arch after repair and to assess the role of timing of assessment and values of ePG in prediction of reintervention.
Materials and methods: All eligible patients for this study who underwent aortic coarctation repair through left thoracotomy from 2001 to 2017 were reviewed. Details of the aortic arch dimensions and associated lesions were obtained by transthoracic echocardiography (TTE). The primary outcome was the ePG across the aortic arch after repair. Longitudinal data analyses with mixed effect modeling were used to determine independent predictors for ePGs.
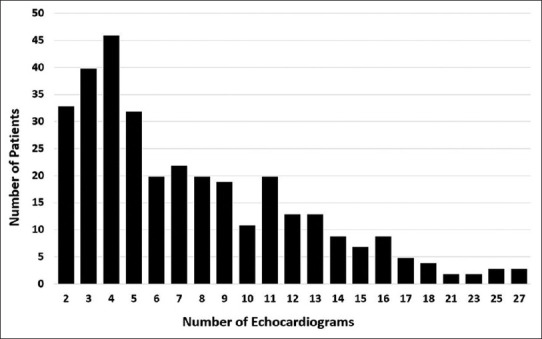
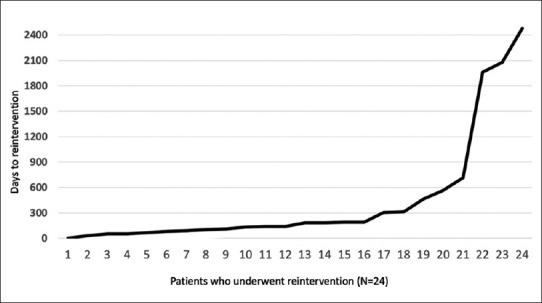
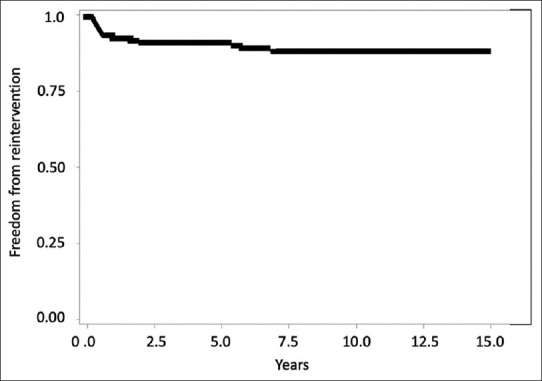
Results: A total of 312 patients were included. Median age and weight were 30 days and 4 kg, respectively. Associated lesions included ventricular septal defect (VSD) (53%), bicuspid aortic valve (53%) and mitral stenosis (25%). Over 15-years follow-up the freedom from reintervention was 92.3%, while 24 out of the 312 patients underwent reintervention (7.7%). Longitudinal data analyses of serial 2566 TTE studies were done. The graphical display showed that the ePG across coarctation area in the first postoperative TTE was the most notable difference between those who underwent reintervention and those who did not. Further testing with proportional hazard and logistic regression modeling confirmed this finding. The area under receiver operating curve statistics showed that an ePG of 25 mmHg is an optimal cutoff value for the prediction of the reintervention.
Conclusions: The ePG acquired in the first postoperative TTE is the most important predictor for reinterventions. The presence of VSD is associated with decreased ePGs. We propose that an ePG in the first postoperative TTE of 25 mmHg or more is a strong predictor for the need of reintervention.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
