{"title":"三振出局和他汀类药物:一个反对在透析患者中使用他汀类药物进行一级预防的案例","authors":"Ali Olyaei PharmD, Edgar V. Lerma MD","doi":"10.1002/dat.20558","DOIUrl":null,"url":null,"abstract":"<p>Cardiovascular disease is the leading cause of death among patients with chronic kidney disease (CKD) and the dialysis population. Approximately 26 million people in the United States are suffering from CKD, with disproportionately higher numbers among patients who have preexisting cardiovascular disease. Vascular abnormalities from hypertension, hyperlipidemia, hyperglycemia, and calcium and phosphate calcifications associated with renal disease rank high among risk factors for early and aggressive causes of accelerated atherosclerosis. It is well known that the risk of cardiovascular events is much higher in dialysis patients compared with the general population; Foly et al. documented that 25- to 35-year-old patients on dialysis are at the same risk of mortality from cardiovascular disease as someone at age 85 from the general population (Figure 1).<span>1</span> Blood cholesterol reduction using HMG-CoA reductase inhibitors (statins) in people at risk of cardiovascular disease has been recommended. In regard to hyperlipidemia and the incidence of cardiovascular disease, most retrospective observations on patients with end-stage renal disease and on dialysis have shown no positive correlation between high cholesterol levels and increased rates of cardiovascular events. In fact, the opposite tendencies have been reported in dialysis patients. A large study with 1,167 HD patients showed that mortality actually increased with cholesterol levels < 140 mg/dL, compared with higher levels, up to 220 mg/dL.<span>2</span> However, this study was not adjusted for disease severity or inflammatory stage associated with late-stage CKD.</p><p>In dialysis patients, most risk factors related to cardiovascular disease have a disconnect between observational studies and interventional studies. Although the effects of lowering low-density lipoprotein cholesterol (LDL-C) on the progression of renal disease or cardiovascular events are not fully understood, it is important to note that only one-fourth of dialysis patients die from acute myocardial infarction (MI). There are now three randomized, placebocontrolled studies of therapy with three different HMG-CoA reductase inhibitors (statins), all with negative results in the dialysis population (Table I).</p><p>The Deutsche Diabetes & Dialysis study (4D) was the first randomized study aimed at investigating the benefits of using a HMG-CoA reductase inhibitor (atorv-astatin) in patients on hemodialysis with type 2 diabetes mellitus.<span>3</span> 4D was a mul-ticenter, randomized, double-blind, pro-spective study of 1,255 (18-80 years old) type 2 diabetes mellitus patients receiv-ing maintenance hemodialysis for less than 2 years. The study was supported by the pharmaceutical industry, and patients were enrolled in 178 centers in Germany. Patients were excluded if the LDL-C was <80 or >190 mg/dL, serum triglycerides were >1,000 mg/dL, liver function tests were abnormal, or they had had a previous cardiovascular event during the previous 3 months.2\n </p><p>A total of 619 patients were enrolled into the atorvastatin 20 mg/d arm of the study, and 636 were given matching pla-cebo. Lipid-lowering agents were discon-tinued upon enrollment, and all eligible subjects were given placebo during a 4-week run-in phase. If LDL-C levels fell below 50 mg/dL, the dose of atorvastatin was reduced to 10 mg/d, and a randomly selected subject from the placebo group would receive an identical dose reduction.</p><p>Data were then recorded every 6 months. This study was started in March 1998 and ran through October 2002. All eligible patients were followed until their final visit in March 2004. Overall, the two groups were similar in baseline characteristics, which included a median level of LDL-C of 121 mg/dL in the atorvastatin group and 125 mg/dL in the placebo group.</p><p>The primary end points were cardio-vascular death, fatal and non-fatal myo-cardial infarction, and stroke. Secondary end points were all-cause mortality and cardiac and cerebrovascular events. At 4 weeks, patients treated with atorvastatin 20 mg daily experienced decreases in LDL-C, total cholesterol, and triglycerides. The mean from baseline to 4 weeks was significantly different in the atorvastatin groups (42%). At median follow-up of 4 years, there were no statistically significant changes in overall primary end points; 12.6% vs. 11.2% at 1 year and 31.9% vs. 30.5% at 3 years in the atorvastatin group vs. the placebo group, respectively. The most serious adverse drug reactions in this study were consistent with age and under-lying medical conditions. However, the incidence of fatal stroke was significantly higher in the atorvastatin-treated group (relative risk of 2.03; 95% CI 1.05-3.93; <i>p</i> = 0.04) compared with placebo.</p><p>A number of editorials questioned the results of the 4D study, i.e., whether the study population selection and the use of atorvastatin were too little and too late in the continuum of underlying disease, or whether the study was not powered to detect the mortality or cardiovascular event differences. In fact, 4D was powered to detect cardiovascular event benefits from the use of statins. Others suggested that the results of the 4D study were not valid because these patients were at higher risk of cardiovascular disease than the general dialysis population, since all patients had a type 2 diabetes diagnosis with normal or low lipid levels.</p><p>The AURORA study (to evaluate the use of rosuvastatin in subjects on regular hemodialysis by assessing survival and car-diovascular events) was aimed at compar-ing the effects of rosuvastatin 10 mg/d with placebo on cardiovascular morbidity and mortality in chronic hemodialysis patients without regard to their baseline lipid status.<span>4</span> AURORA was a double-blind, random-ized, placebo-controlled, multicenter trial. A total of 2,776 patients were enrolled from 25 countries. Unfortunately, AURORA included only dialysis patients between 50 and 80 years old on dialysis for more than 3 months. Those excluded were patients who had used statins within the previous 6 months, those with elevated liver function tests or creatinine kinase > 3X ULN, or uncontrolled hypothyroidism verified by a thyroid-stimulating hormone (TSH) level of >1.5X ULN. Patients initially entered a 2-week screening period and were then randomized in blocks of four in a 1:1 ratio to rosuvastatin 10 mg or placebo. A total of 1,389 patients were assigned rosuvastatin 10 mg/d, and 1,384 received matching pla-cebo. The median follow-up was 3.8 years, with visits every 3 months during the study period. The primary end point was time to major cardiovascular events, which included fatal and non-fatal myocardial infarction and stroke. Secondary end points included all-cause mortality, cardiovascular event-free survival, revascularization, and death from cardiovascular and non-cardio-vascular causes. Change in baseline lipids and high sensitivity to C-reactive protein (CRP) were tertiary end points.</p><p>Baseline LDL-C levels in the rosuvas-tatin and placebo groups were 100 and 99 mg/dL, respectively. Overall baseline char-acteristics were evenly distributed among the two groups. The mean duration of study medication was 2.4 years, with a mean length of follow-up of 3.2 years. A total of 1,296 patients died during the study, and another 810 patients discontinued the treat-ment because of adverse drug reactions or renal transplantation (a total of 2,106 patients). Within the first year, LDL-C was reduced by a mean of about 43% in the rosuvastatin group, and high-sensitivity (hs)-CRP decreased by 11.5% in patients taking the statin. No statistically significant changes in mortality or primary or second-ary end points were observed for any treat-ment arms. This finding was consistent in all predefined subgroup analyses including patients with diabetes at baseline. Major cardiovascular events combined were 9.2% in 396 rosuvastatin group patients vs. 9.5% in 405 placebo group patients (hazard ratio 0.96; 95% CI 0.84-1.11; <i>p</i> = 0.59). The all-cause mortality rate of rosuvastatin vs. the placebo group (13.5 rosuvastatin vs. 14.0 placebo events per 100 patient-years; hazard ratio 0.96; 95% CI 0.86-1.07; <i>p</i> = 0.51) was also insignificant. No clinically important differences between the groups were observed for safety parameters; how-ever, similar to the 4D study, an increased rate of fatal stroke (hemorrhagic stroke) was noted in the rosuvastatin arm of the study in patients with diabetes (12 in the rosuvastatin group vs. 2 in placebo group; <i>p</i> = 0.03).</p><p>The last study is the Study of Heart and Renal Protection (SHARP). This was a randomized controlled trial to determine the benefits of cholesterol-lowering treatment in patients with CKD and on dialysis.<span>5</span> SHARP was sponsored, designed, run, and analyzed by the Oxford University. Funding was provided by a pharmaceutical firm, the UK Medical Research Council (MRC), the British Heart Foundation, and the Australian National Health MRC. The trial was guided by an independent steering committee of nephrologists.</p><p>Results of the SHARP study were recently presented at an international meet-ing [http://www.ctsu.ox.ac.uk/∼sharp/slides. htm]. A total of 9,270 patients with chronic kidney disease and 3,023 dialysis patients were randomized to simvastatin 20 mg/d plus ezetimibe 10 mg or placebo. Patients with previous cardiovascular disease were excluded. The median follow-up was 4.9 years. Baseline LDL-C levels were 108 mg/ dL for all patients and 100 mg/dL for dialysis patients. LDL-C was reduced at 1 year after 30 mg/dL with simvastatin 20 mg alone and after 43 mg/dL with simvastatin 20 mg/d plus ezetimibe 10 mg. Like the two previous studies, baseline characteristics were evenly distributed among the two groups. The objective of the SHARP study was to investigate whether lowering LDL-C may prevent “major vascular events” (i.e., fatal or non-fatal strokes, non-fatal myocardial infarction or cardiac death, and operations to unblock arteries) or slow the progression of CKD in dialysis patients with CKD. The esti-mated glomerular filtration rate (eGFR) for both groups was approximately 27 mL/min/1.73 m<sup>2</sup>.</p><p>The primary end points were the occurrence of a major atherosclerotic event that included coronary death, myocardial infarction, non-hemorrhagic stroke, or the need for revascularization procedures. Initially, patients underwent a 6-week placebo trial run-in to help determine those likely to be compliant. In the fi rst year, all patients were randomized to placebo or simvastatin 20 mg daily. After 1 year, patients were randomized to a placebo-combination or an ezetimibe/simvastatin combination. Postrandomization follow-up was conducted at 2 and 6 months, and then biannually for at least 4 years. The overall result was signifi - cant for the reduction of major atherosclerotic events by 17% in the simvastatin and ezetimibe treatment arm compared with placebo (relative risk 0.83; 95% CI 0.74, 0.94; log rank P¼0.002]. However, neither a clinical nor a statistically signifi cant reduction in mortality rates or cardiovascular events was observed in the dialysis population (15% vs. 16.5%). The results of the SHARP study for patients on dialysis were similar to those of AURORA and 4D studies. The number needed to treat for dialysis is 67 patients for 5 years to avoid one cardiovascular event. At the cost of $145 per month of ezetimibe/simvastatin combination for 5 years, it cost over $500,000 to avoid one cardiovascular event. This risk reduction can be accomplished by other, much less expensive methods.</p><p>The results of the SHARP study have received a fair amount of attention in the general media. Recommendations in press releases have been misleading, and this study should not be extrapolated to the general population or dialysis patients. In addition, the SHARP study did not compare simvastatin vs. the combination of simvastatin plus ezetimibe. This study did not shed any light on controversies related to the use of an expensive drug like ezetimibe without any long-term cardiovascular benefi t. Two separate studies of ezetimibe use in the past have not shown any reduction in major clinical end points compared with placebo or niacin.<span>6</span>, <span>7</span> Similarly, in the two previous studies, SHARP was designed and powered to detect any mortality and cardiovascular events benefi ts from the use of statins. Regardless, no benefi t was noted.</p><p>Prevention of cardiovascular disease in dialysis patients requires identifi cation of major risk factors and a reduction in global cardiovascular risk factors. Although hyperlipidemia-related cardiovascular events are important risk factors—accentuated by other risk factors and patient characteristics—most hyperlipidemia studies are sponsored by pharmaceutical companies, and the results have, in part, been misleading. The use of statins in dialysis patients continues to rise, and the results of these studies have very limited impact on prescribing patterns. Finally, a new metaanalysis has cast new doubt on the value of statins in primary prevention.<span>8</span>, <span>9</span> Taylor and co-workers reviewed 16 studies with over 34,000 patients and reported very limited long-term benefi ts. This review from available randomized clinical trials did not demonstrate that aggressive lipid lowering in low-risk patient populations may provide any clinical benefi t compared with other patients without statin exposure.</p><p>The results of three large, welldesigned clinical studies and new published data from Cochran indicate that statins have a very limited role in primary prevention for dialysis and low-risk patients. Therefore, three strikes and statins are out for the primary prevention of cardiovascular disease in dialysis patients.</p>","PeriodicalId":51012,"journal":{"name":"Dialysis & Transplantation","volume":"40 4","pages":"148-151"},"PeriodicalIF":0.0000,"publicationDate":"2011-04-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/dat.20558","citationCount":"0","resultStr":"{\"title\":\"Three strikes and statins out: A case against use of statins in dialysis patients for primary prevention\",\"authors\":\"Ali Olyaei PharmD, Edgar V. Lerma MD\",\"doi\":\"10.1002/dat.20558\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Cardiovascular disease is the leading cause of death among patients with chronic kidney disease (CKD) and the dialysis population. Approximately 26 million people in the United States are suffering from CKD, with disproportionately higher numbers among patients who have preexisting cardiovascular disease. Vascular abnormalities from hypertension, hyperlipidemia, hyperglycemia, and calcium and phosphate calcifications associated with renal disease rank high among risk factors for early and aggressive causes of accelerated atherosclerosis. It is well known that the risk of cardiovascular events is much higher in dialysis patients compared with the general population; Foly et al. documented that 25- to 35-year-old patients on dialysis are at the same risk of mortality from cardiovascular disease as someone at age 85 from the general population (Figure 1).<span>1</span> Blood cholesterol reduction using HMG-CoA reductase inhibitors (statins) in people at risk of cardiovascular disease has been recommended. In regard to hyperlipidemia and the incidence of cardiovascular disease, most retrospective observations on patients with end-stage renal disease and on dialysis have shown no positive correlation between high cholesterol levels and increased rates of cardiovascular events. In fact, the opposite tendencies have been reported in dialysis patients. A large study with 1,167 HD patients showed that mortality actually increased with cholesterol levels < 140 mg/dL, compared with higher levels, up to 220 mg/dL.<span>2</span> However, this study was not adjusted for disease severity or inflammatory stage associated with late-stage CKD.</p><p>In dialysis patients, most risk factors related to cardiovascular disease have a disconnect between observational studies and interventional studies. Although the effects of lowering low-density lipoprotein cholesterol (LDL-C) on the progression of renal disease or cardiovascular events are not fully understood, it is important to note that only one-fourth of dialysis patients die from acute myocardial infarction (MI). There are now three randomized, placebocontrolled studies of therapy with three different HMG-CoA reductase inhibitors (statins), all with negative results in the dialysis population (Table I).</p><p>The Deutsche Diabetes & Dialysis study (4D) was the first randomized study aimed at investigating the benefits of using a HMG-CoA reductase inhibitor (atorv-astatin) in patients on hemodialysis with type 2 diabetes mellitus.<span>3</span> 4D was a mul-ticenter, randomized, double-blind, pro-spective study of 1,255 (18-80 years old) type 2 diabetes mellitus patients receiv-ing maintenance hemodialysis for less than 2 years. The study was supported by the pharmaceutical industry, and patients were enrolled in 178 centers in Germany. Patients were excluded if the LDL-C was <80 or >190 mg/dL, serum triglycerides were >1,000 mg/dL, liver function tests were abnormal, or they had had a previous cardiovascular event during the previous 3 months.2\\n </p><p>A total of 619 patients were enrolled into the atorvastatin 20 mg/d arm of the study, and 636 were given matching pla-cebo. Lipid-lowering agents were discon-tinued upon enrollment, and all eligible subjects were given placebo during a 4-week run-in phase. If LDL-C levels fell below 50 mg/dL, the dose of atorvastatin was reduced to 10 mg/d, and a randomly selected subject from the placebo group would receive an identical dose reduction.</p><p>Data were then recorded every 6 months. This study was started in March 1998 and ran through October 2002. All eligible patients were followed until their final visit in March 2004. Overall, the two groups were similar in baseline characteristics, which included a median level of LDL-C of 121 mg/dL in the atorvastatin group and 125 mg/dL in the placebo group.</p><p>The primary end points were cardio-vascular death, fatal and non-fatal myo-cardial infarction, and stroke. Secondary end points were all-cause mortality and cardiac and cerebrovascular events. At 4 weeks, patients treated with atorvastatin 20 mg daily experienced decreases in LDL-C, total cholesterol, and triglycerides. The mean from baseline to 4 weeks was significantly different in the atorvastatin groups (42%). At median follow-up of 4 years, there were no statistically significant changes in overall primary end points; 12.6% vs. 11.2% at 1 year and 31.9% vs. 30.5% at 3 years in the atorvastatin group vs. the placebo group, respectively. The most serious adverse drug reactions in this study were consistent with age and under-lying medical conditions. However, the incidence of fatal stroke was significantly higher in the atorvastatin-treated group (relative risk of 2.03; 95% CI 1.05-3.93; <i>p</i> = 0.04) compared with placebo.</p><p>A number of editorials questioned the results of the 4D study, i.e., whether the study population selection and the use of atorvastatin were too little and too late in the continuum of underlying disease, or whether the study was not powered to detect the mortality or cardiovascular event differences. In fact, 4D was powered to detect cardiovascular event benefits from the use of statins. Others suggested that the results of the 4D study were not valid because these patients were at higher risk of cardiovascular disease than the general dialysis population, since all patients had a type 2 diabetes diagnosis with normal or low lipid levels.</p><p>The AURORA study (to evaluate the use of rosuvastatin in subjects on regular hemodialysis by assessing survival and car-diovascular events) was aimed at compar-ing the effects of rosuvastatin 10 mg/d with placebo on cardiovascular morbidity and mortality in chronic hemodialysis patients without regard to their baseline lipid status.<span>4</span> AURORA was a double-blind, random-ized, placebo-controlled, multicenter trial. A total of 2,776 patients were enrolled from 25 countries. Unfortunately, AURORA included only dialysis patients between 50 and 80 years old on dialysis for more than 3 months. Those excluded were patients who had used statins within the previous 6 months, those with elevated liver function tests or creatinine kinase > 3X ULN, or uncontrolled hypothyroidism verified by a thyroid-stimulating hormone (TSH) level of >1.5X ULN. Patients initially entered a 2-week screening period and were then randomized in blocks of four in a 1:1 ratio to rosuvastatin 10 mg or placebo. A total of 1,389 patients were assigned rosuvastatin 10 mg/d, and 1,384 received matching pla-cebo. The median follow-up was 3.8 years, with visits every 3 months during the study period. The primary end point was time to major cardiovascular events, which included fatal and non-fatal myocardial infarction and stroke. Secondary end points included all-cause mortality, cardiovascular event-free survival, revascularization, and death from cardiovascular and non-cardio-vascular causes. Change in baseline lipids and high sensitivity to C-reactive protein (CRP) were tertiary end points.</p><p>Baseline LDL-C levels in the rosuvas-tatin and placebo groups were 100 and 99 mg/dL, respectively. Overall baseline char-acteristics were evenly distributed among the two groups. The mean duration of study medication was 2.4 years, with a mean length of follow-up of 3.2 years. A total of 1,296 patients died during the study, and another 810 patients discontinued the treat-ment because of adverse drug reactions or renal transplantation (a total of 2,106 patients). Within the first year, LDL-C was reduced by a mean of about 43% in the rosuvastatin group, and high-sensitivity (hs)-CRP decreased by 11.5% in patients taking the statin. No statistically significant changes in mortality or primary or second-ary end points were observed for any treat-ment arms. This finding was consistent in all predefined subgroup analyses including patients with diabetes at baseline. Major cardiovascular events combined were 9.2% in 396 rosuvastatin group patients vs. 9.5% in 405 placebo group patients (hazard ratio 0.96; 95% CI 0.84-1.11; <i>p</i> = 0.59). The all-cause mortality rate of rosuvastatin vs. the placebo group (13.5 rosuvastatin vs. 14.0 placebo events per 100 patient-years; hazard ratio 0.96; 95% CI 0.86-1.07; <i>p</i> = 0.51) was also insignificant. No clinically important differences between the groups were observed for safety parameters; how-ever, similar to the 4D study, an increased rate of fatal stroke (hemorrhagic stroke) was noted in the rosuvastatin arm of the study in patients with diabetes (12 in the rosuvastatin group vs. 2 in placebo group; <i>p</i> = 0.03).</p><p>The last study is the Study of Heart and Renal Protection (SHARP). This was a randomized controlled trial to determine the benefits of cholesterol-lowering treatment in patients with CKD and on dialysis.<span>5</span> SHARP was sponsored, designed, run, and analyzed by the Oxford University. Funding was provided by a pharmaceutical firm, the UK Medical Research Council (MRC), the British Heart Foundation, and the Australian National Health MRC. The trial was guided by an independent steering committee of nephrologists.</p><p>Results of the SHARP study were recently presented at an international meet-ing [http://www.ctsu.ox.ac.uk/∼sharp/slides. htm]. A total of 9,270 patients with chronic kidney disease and 3,023 dialysis patients were randomized to simvastatin 20 mg/d plus ezetimibe 10 mg or placebo. Patients with previous cardiovascular disease were excluded. The median follow-up was 4.9 years. Baseline LDL-C levels were 108 mg/ dL for all patients and 100 mg/dL for dialysis patients. LDL-C was reduced at 1 year after 30 mg/dL with simvastatin 20 mg alone and after 43 mg/dL with simvastatin 20 mg/d plus ezetimibe 10 mg. Like the two previous studies, baseline characteristics were evenly distributed among the two groups. The objective of the SHARP study was to investigate whether lowering LDL-C may prevent “major vascular events” (i.e., fatal or non-fatal strokes, non-fatal myocardial infarction or cardiac death, and operations to unblock arteries) or slow the progression of CKD in dialysis patients with CKD. The esti-mated glomerular filtration rate (eGFR) for both groups was approximately 27 mL/min/1.73 m<sup>2</sup>.</p><p>The primary end points were the occurrence of a major atherosclerotic event that included coronary death, myocardial infarction, non-hemorrhagic stroke, or the need for revascularization procedures. Initially, patients underwent a 6-week placebo trial run-in to help determine those likely to be compliant. In the fi rst year, all patients were randomized to placebo or simvastatin 20 mg daily. After 1 year, patients were randomized to a placebo-combination or an ezetimibe/simvastatin combination. Postrandomization follow-up was conducted at 2 and 6 months, and then biannually for at least 4 years. The overall result was signifi - cant for the reduction of major atherosclerotic events by 17% in the simvastatin and ezetimibe treatment arm compared with placebo (relative risk 0.83; 95% CI 0.74, 0.94; log rank P¼0.002]. However, neither a clinical nor a statistically signifi cant reduction in mortality rates or cardiovascular events was observed in the dialysis population (15% vs. 16.5%). The results of the SHARP study for patients on dialysis were similar to those of AURORA and 4D studies. The number needed to treat for dialysis is 67 patients for 5 years to avoid one cardiovascular event. At the cost of $145 per month of ezetimibe/simvastatin combination for 5 years, it cost over $500,000 to avoid one cardiovascular event. This risk reduction can be accomplished by other, much less expensive methods.</p><p>The results of the SHARP study have received a fair amount of attention in the general media. Recommendations in press releases have been misleading, and this study should not be extrapolated to the general population or dialysis patients. In addition, the SHARP study did not compare simvastatin vs. the combination of simvastatin plus ezetimibe. This study did not shed any light on controversies related to the use of an expensive drug like ezetimibe without any long-term cardiovascular benefi t. Two separate studies of ezetimibe use in the past have not shown any reduction in major clinical end points compared with placebo or niacin.<span>6</span>, <span>7</span> Similarly, in the two previous studies, SHARP was designed and powered to detect any mortality and cardiovascular events benefi ts from the use of statins. Regardless, no benefi t was noted.</p><p>Prevention of cardiovascular disease in dialysis patients requires identifi cation of major risk factors and a reduction in global cardiovascular risk factors. Although hyperlipidemia-related cardiovascular events are important risk factors—accentuated by other risk factors and patient characteristics—most hyperlipidemia studies are sponsored by pharmaceutical companies, and the results have, in part, been misleading. The use of statins in dialysis patients continues to rise, and the results of these studies have very limited impact on prescribing patterns. Finally, a new metaanalysis has cast new doubt on the value of statins in primary prevention.<span>8</span>, <span>9</span> Taylor and co-workers reviewed 16 studies with over 34,000 patients and reported very limited long-term benefi ts. This review from available randomized clinical trials did not demonstrate that aggressive lipid lowering in low-risk patient populations may provide any clinical benefi t compared with other patients without statin exposure.</p><p>The results of three large, welldesigned clinical studies and new published data from Cochran indicate that statins have a very limited role in primary prevention for dialysis and low-risk patients. Therefore, three strikes and statins are out for the primary prevention of cardiovascular disease in dialysis patients.</p>\",\"PeriodicalId\":51012,\"journal\":{\"name\":\"Dialysis & Transplantation\",\"volume\":\"40 4\",\"pages\":\"148-151\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2011-04-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1002/dat.20558\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Dialysis & Transplantation\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/dat.20558\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Dialysis & Transplantation","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/dat.20558","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Three strikes and statins out: A case against use of statins in dialysis patients for primary prevention
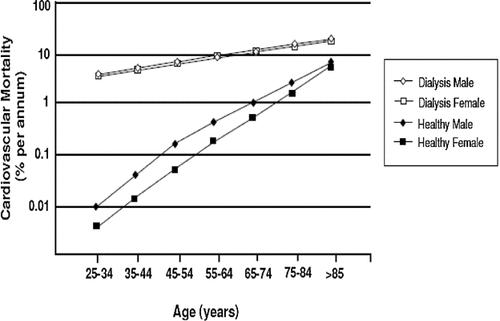
Cardiovascular disease is the leading cause of death among patients with chronic kidney disease (CKD) and the dialysis population. Approximately 26 million people in the United States are suffering from CKD, with disproportionately higher numbers among patients who have preexisting cardiovascular disease. Vascular abnormalities from hypertension, hyperlipidemia, hyperglycemia, and calcium and phosphate calcifications associated with renal disease rank high among risk factors for early and aggressive causes of accelerated atherosclerosis. It is well known that the risk of cardiovascular events is much higher in dialysis patients compared with the general population; Foly et al. documented that 25- to 35-year-old patients on dialysis are at the same risk of mortality from cardiovascular disease as someone at age 85 from the general population (Figure 1).1 Blood cholesterol reduction using HMG-CoA reductase inhibitors (statins) in people at risk of cardiovascular disease has been recommended. In regard to hyperlipidemia and the incidence of cardiovascular disease, most retrospective observations on patients with end-stage renal disease and on dialysis have shown no positive correlation between high cholesterol levels and increased rates of cardiovascular events. In fact, the opposite tendencies have been reported in dialysis patients. A large study with 1,167 HD patients showed that mortality actually increased with cholesterol levels < 140 mg/dL, compared with higher levels, up to 220 mg/dL.2 However, this study was not adjusted for disease severity or inflammatory stage associated with late-stage CKD.
In dialysis patients, most risk factors related to cardiovascular disease have a disconnect between observational studies and interventional studies. Although the effects of lowering low-density lipoprotein cholesterol (LDL-C) on the progression of renal disease or cardiovascular events are not fully understood, it is important to note that only one-fourth of dialysis patients die from acute myocardial infarction (MI). There are now three randomized, placebocontrolled studies of therapy with three different HMG-CoA reductase inhibitors (statins), all with negative results in the dialysis population (Table I).
The Deutsche Diabetes & Dialysis study (4D) was the first randomized study aimed at investigating the benefits of using a HMG-CoA reductase inhibitor (atorv-astatin) in patients on hemodialysis with type 2 diabetes mellitus.3 4D was a mul-ticenter, randomized, double-blind, pro-spective study of 1,255 (18-80 years old) type 2 diabetes mellitus patients receiv-ing maintenance hemodialysis for less than 2 years. The study was supported by the pharmaceutical industry, and patients were enrolled in 178 centers in Germany. Patients were excluded if the LDL-C was <80 or >190 mg/dL, serum triglycerides were >1,000 mg/dL, liver function tests were abnormal, or they had had a previous cardiovascular event during the previous 3 months.2
A total of 619 patients were enrolled into the atorvastatin 20 mg/d arm of the study, and 636 were given matching pla-cebo. Lipid-lowering agents were discon-tinued upon enrollment, and all eligible subjects were given placebo during a 4-week run-in phase. If LDL-C levels fell below 50 mg/dL, the dose of atorvastatin was reduced to 10 mg/d, and a randomly selected subject from the placebo group would receive an identical dose reduction.
Data were then recorded every 6 months. This study was started in March 1998 and ran through October 2002. All eligible patients were followed until their final visit in March 2004. Overall, the two groups were similar in baseline characteristics, which included a median level of LDL-C of 121 mg/dL in the atorvastatin group and 125 mg/dL in the placebo group.
The primary end points were cardio-vascular death, fatal and non-fatal myo-cardial infarction, and stroke. Secondary end points were all-cause mortality and cardiac and cerebrovascular events. At 4 weeks, patients treated with atorvastatin 20 mg daily experienced decreases in LDL-C, total cholesterol, and triglycerides. The mean from baseline to 4 weeks was significantly different in the atorvastatin groups (42%). At median follow-up of 4 years, there were no statistically significant changes in overall primary end points; 12.6% vs. 11.2% at 1 year and 31.9% vs. 30.5% at 3 years in the atorvastatin group vs. the placebo group, respectively. The most serious adverse drug reactions in this study were consistent with age and under-lying medical conditions. However, the incidence of fatal stroke was significantly higher in the atorvastatin-treated group (relative risk of 2.03; 95% CI 1.05-3.93; p = 0.04) compared with placebo.
A number of editorials questioned the results of the 4D study, i.e., whether the study population selection and the use of atorvastatin were too little and too late in the continuum of underlying disease, or whether the study was not powered to detect the mortality or cardiovascular event differences. In fact, 4D was powered to detect cardiovascular event benefits from the use of statins. Others suggested that the results of the 4D study were not valid because these patients were at higher risk of cardiovascular disease than the general dialysis population, since all patients had a type 2 diabetes diagnosis with normal or low lipid levels.
The AURORA study (to evaluate the use of rosuvastatin in subjects on regular hemodialysis by assessing survival and car-diovascular events) was aimed at compar-ing the effects of rosuvastatin 10 mg/d with placebo on cardiovascular morbidity and mortality in chronic hemodialysis patients without regard to their baseline lipid status.4 AURORA was a double-blind, random-ized, placebo-controlled, multicenter trial. A total of 2,776 patients were enrolled from 25 countries. Unfortunately, AURORA included only dialysis patients between 50 and 80 years old on dialysis for more than 3 months. Those excluded were patients who had used statins within the previous 6 months, those with elevated liver function tests or creatinine kinase > 3X ULN, or uncontrolled hypothyroidism verified by a thyroid-stimulating hormone (TSH) level of >1.5X ULN. Patients initially entered a 2-week screening period and were then randomized in blocks of four in a 1:1 ratio to rosuvastatin 10 mg or placebo. A total of 1,389 patients were assigned rosuvastatin 10 mg/d, and 1,384 received matching pla-cebo. The median follow-up was 3.8 years, with visits every 3 months during the study period. The primary end point was time to major cardiovascular events, which included fatal and non-fatal myocardial infarction and stroke. Secondary end points included all-cause mortality, cardiovascular event-free survival, revascularization, and death from cardiovascular and non-cardio-vascular causes. Change in baseline lipids and high sensitivity to C-reactive protein (CRP) were tertiary end points.
Baseline LDL-C levels in the rosuvas-tatin and placebo groups were 100 and 99 mg/dL, respectively. Overall baseline char-acteristics were evenly distributed among the two groups. The mean duration of study medication was 2.4 years, with a mean length of follow-up of 3.2 years. A total of 1,296 patients died during the study, and another 810 patients discontinued the treat-ment because of adverse drug reactions or renal transplantation (a total of 2,106 patients). Within the first year, LDL-C was reduced by a mean of about 43% in the rosuvastatin group, and high-sensitivity (hs)-CRP decreased by 11.5% in patients taking the statin. No statistically significant changes in mortality or primary or second-ary end points were observed for any treat-ment arms. This finding was consistent in all predefined subgroup analyses including patients with diabetes at baseline. Major cardiovascular events combined were 9.2% in 396 rosuvastatin group patients vs. 9.5% in 405 placebo group patients (hazard ratio 0.96; 95% CI 0.84-1.11; p = 0.59). The all-cause mortality rate of rosuvastatin vs. the placebo group (13.5 rosuvastatin vs. 14.0 placebo events per 100 patient-years; hazard ratio 0.96; 95% CI 0.86-1.07; p = 0.51) was also insignificant. No clinically important differences between the groups were observed for safety parameters; how-ever, similar to the 4D study, an increased rate of fatal stroke (hemorrhagic stroke) was noted in the rosuvastatin arm of the study in patients with diabetes (12 in the rosuvastatin group vs. 2 in placebo group; p = 0.03).
The last study is the Study of Heart and Renal Protection (SHARP). This was a randomized controlled trial to determine the benefits of cholesterol-lowering treatment in patients with CKD and on dialysis.5 SHARP was sponsored, designed, run, and analyzed by the Oxford University. Funding was provided by a pharmaceutical firm, the UK Medical Research Council (MRC), the British Heart Foundation, and the Australian National Health MRC. The trial was guided by an independent steering committee of nephrologists.
Results of the SHARP study were recently presented at an international meet-ing [http://www.ctsu.ox.ac.uk/∼sharp/slides. htm]. A total of 9,270 patients with chronic kidney disease and 3,023 dialysis patients were randomized to simvastatin 20 mg/d plus ezetimibe 10 mg or placebo. Patients with previous cardiovascular disease were excluded. The median follow-up was 4.9 years. Baseline LDL-C levels were 108 mg/ dL for all patients and 100 mg/dL for dialysis patients. LDL-C was reduced at 1 year after 30 mg/dL with simvastatin 20 mg alone and after 43 mg/dL with simvastatin 20 mg/d plus ezetimibe 10 mg. Like the two previous studies, baseline characteristics were evenly distributed among the two groups. The objective of the SHARP study was to investigate whether lowering LDL-C may prevent “major vascular events” (i.e., fatal or non-fatal strokes, non-fatal myocardial infarction or cardiac death, and operations to unblock arteries) or slow the progression of CKD in dialysis patients with CKD. The esti-mated glomerular filtration rate (eGFR) for both groups was approximately 27 mL/min/1.73 m2.
The primary end points were the occurrence of a major atherosclerotic event that included coronary death, myocardial infarction, non-hemorrhagic stroke, or the need for revascularization procedures. Initially, patients underwent a 6-week placebo trial run-in to help determine those likely to be compliant. In the fi rst year, all patients were randomized to placebo or simvastatin 20 mg daily. After 1 year, patients were randomized to a placebo-combination or an ezetimibe/simvastatin combination. Postrandomization follow-up was conducted at 2 and 6 months, and then biannually for at least 4 years. The overall result was signifi - cant for the reduction of major atherosclerotic events by 17% in the simvastatin and ezetimibe treatment arm compared with placebo (relative risk 0.83; 95% CI 0.74, 0.94; log rank P¼0.002]. However, neither a clinical nor a statistically signifi cant reduction in mortality rates or cardiovascular events was observed in the dialysis population (15% vs. 16.5%). The results of the SHARP study for patients on dialysis were similar to those of AURORA and 4D studies. The number needed to treat for dialysis is 67 patients for 5 years to avoid one cardiovascular event. At the cost of $145 per month of ezetimibe/simvastatin combination for 5 years, it cost over $500,000 to avoid one cardiovascular event. This risk reduction can be accomplished by other, much less expensive methods.
The results of the SHARP study have received a fair amount of attention in the general media. Recommendations in press releases have been misleading, and this study should not be extrapolated to the general population or dialysis patients. In addition, the SHARP study did not compare simvastatin vs. the combination of simvastatin plus ezetimibe. This study did not shed any light on controversies related to the use of an expensive drug like ezetimibe without any long-term cardiovascular benefi t. Two separate studies of ezetimibe use in the past have not shown any reduction in major clinical end points compared with placebo or niacin.6, 7 Similarly, in the two previous studies, SHARP was designed and powered to detect any mortality and cardiovascular events benefi ts from the use of statins. Regardless, no benefi t was noted.
Prevention of cardiovascular disease in dialysis patients requires identifi cation of major risk factors and a reduction in global cardiovascular risk factors. Although hyperlipidemia-related cardiovascular events are important risk factors—accentuated by other risk factors and patient characteristics—most hyperlipidemia studies are sponsored by pharmaceutical companies, and the results have, in part, been misleading. The use of statins in dialysis patients continues to rise, and the results of these studies have very limited impact on prescribing patterns. Finally, a new metaanalysis has cast new doubt on the value of statins in primary prevention.8, 9 Taylor and co-workers reviewed 16 studies with over 34,000 patients and reported very limited long-term benefi ts. This review from available randomized clinical trials did not demonstrate that aggressive lipid lowering in low-risk patient populations may provide any clinical benefi t compared with other patients without statin exposure.
The results of three large, welldesigned clinical studies and new published data from Cochran indicate that statins have a very limited role in primary prevention for dialysis and low-risk patients. Therefore, three strikes and statins are out for the primary prevention of cardiovascular disease in dialysis patients.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
