Michael Doppler, Christin Fürnstahl, Simone Hammer, Michael Melter, Niklas Verloh, Hans Jürgen Schlitt, Wibke Uller
{"title":"经皮肝内胆管引流治疗小儿肝移植术后胆漏——病例系列。","authors":"Michael Doppler, Christin Fürnstahl, Simone Hammer, Michael Melter, Niklas Verloh, Hans Jürgen Schlitt, Wibke Uller","doi":"10.3390/tomography9050153","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Biliary leaks are a severe complication after pediatric liver transplantation (pLT), and successful management is challenging.</p><p><strong>Objectives: </strong>The aim of this case series was to assess the outcome of percutaneous transhepatic biliary drainage (PTBD) in children with bile leaks following pLT. The necessity of additional percutaneous bilioma drainage and laboratory changes during therapy and follow-up was documented.</p><p><strong>Material and methods: </strong>All children who underwent PTBD for biliary leak following pLT were included in this consecutive retrospective single-center study and analyzed regarding site of leak, management of additional bilioma, treatment response, and patient and transplant survival. The courses of inflammation, cholestasis parameters, and liver enzymes were retrospectively reviewed.</p><p><strong>Results: </strong>Ten children underwent PTBD treatment for biliary leak after pLT. Seven patients presented with leakage at the hepaticojejunostomy, two with leakage at the choledocho-choledochostomy and one with a bile leak because of an overlooked segmental bile duct. In terms of the mean, the PTBD treatment started 40.3 ± 31.7 days after pLT. The mean duration of PTBD treatment was 109.7 ± 103.6 days. Additional percutaneous bilioma drainage was required in eight cases. Bile leak treatment was successful in all cases, and no complications occurred. The patient and transplant survival rate was 100%. CRP serum level, leukocyte count, gamma-glutamyl transferase (GGT), and total and direct bilirubin level decreased significantly during treatment with a very strong effect size. Additionally, the gamma-glutamyl transferase level showed a statistically significant reduction during follow-up.</p><p><strong>Conclusions: </strong>PTBD is a very successful strategy for bile leak therapy after pLT.</p>","PeriodicalId":51330,"journal":{"name":"Tomography","volume":"9 5","pages":"1965-1975"},"PeriodicalIF":2.2000,"publicationDate":"2023-10-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10610565/pdf/","citationCount":"0","resultStr":"{\"title\":\"Biliary Leak after Pediatric Liver Transplantation Treated by Percutaneous Transhepatic Biliary Drainage-A Case Series.\",\"authors\":\"Michael Doppler, Christin Fürnstahl, Simone Hammer, Michael Melter, Niklas Verloh, Hans Jürgen Schlitt, Wibke Uller\",\"doi\":\"10.3390/tomography9050153\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Biliary leaks are a severe complication after pediatric liver transplantation (pLT), and successful management is challenging.</p><p><strong>Objectives: </strong>The aim of this case series was to assess the outcome of percutaneous transhepatic biliary drainage (PTBD) in children with bile leaks following pLT. The necessity of additional percutaneous bilioma drainage and laboratory changes during therapy and follow-up was documented.</p><p><strong>Material and methods: </strong>All children who underwent PTBD for biliary leak following pLT were included in this consecutive retrospective single-center study and analyzed regarding site of leak, management of additional bilioma, treatment response, and patient and transplant survival. The courses of inflammation, cholestasis parameters, and liver enzymes were retrospectively reviewed.</p><p><strong>Results: </strong>Ten children underwent PTBD treatment for biliary leak after pLT. Seven patients presented with leakage at the hepaticojejunostomy, two with leakage at the choledocho-choledochostomy and one with a bile leak because of an overlooked segmental bile duct. In terms of the mean, the PTBD treatment started 40.3 ± 31.7 days after pLT. The mean duration of PTBD treatment was 109.7 ± 103.6 days. Additional percutaneous bilioma drainage was required in eight cases. Bile leak treatment was successful in all cases, and no complications occurred. The patient and transplant survival rate was 100%. CRP serum level, leukocyte count, gamma-glutamyl transferase (GGT), and total and direct bilirubin level decreased significantly during treatment with a very strong effect size. Additionally, the gamma-glutamyl transferase level showed a statistically significant reduction during follow-up.</p><p><strong>Conclusions: </strong>PTBD is a very successful strategy for bile leak therapy after pLT.</p>\",\"PeriodicalId\":51330,\"journal\":{\"name\":\"Tomography\",\"volume\":\"9 5\",\"pages\":\"1965-1975\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2023-10-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10610565/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Tomography\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3390/tomography9050153\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tomography","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/tomography9050153","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Biliary Leak after Pediatric Liver Transplantation Treated by Percutaneous Transhepatic Biliary Drainage-A Case Series.
Background: Biliary leaks are a severe complication after pediatric liver transplantation (pLT), and successful management is challenging.
Objectives: The aim of this case series was to assess the outcome of percutaneous transhepatic biliary drainage (PTBD) in children with bile leaks following pLT. The necessity of additional percutaneous bilioma drainage and laboratory changes during therapy and follow-up was documented.
Material and methods: All children who underwent PTBD for biliary leak following pLT were included in this consecutive retrospective single-center study and analyzed regarding site of leak, management of additional bilioma, treatment response, and patient and transplant survival. The courses of inflammation, cholestasis parameters, and liver enzymes were retrospectively reviewed.
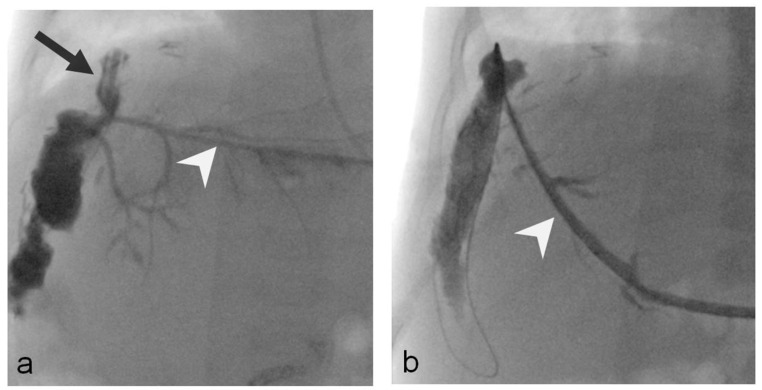
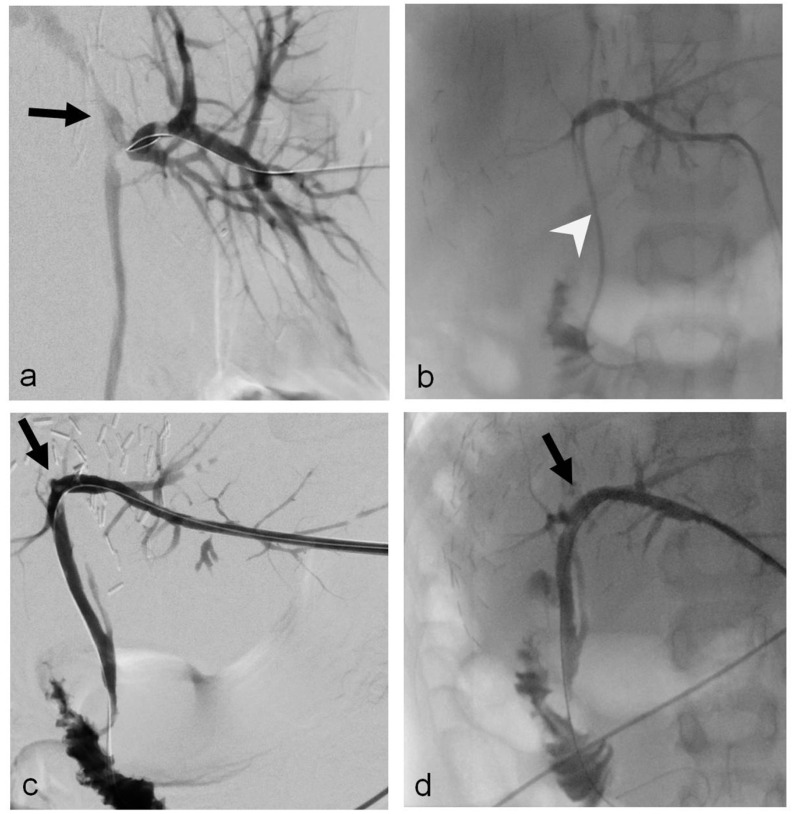
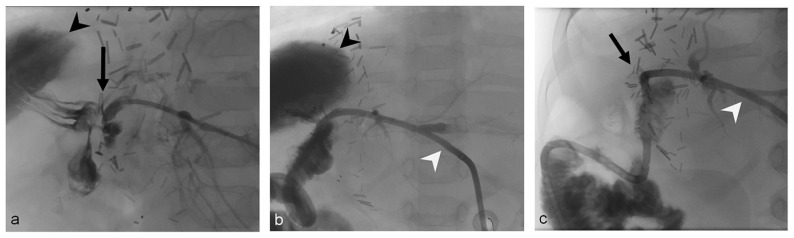
Results: Ten children underwent PTBD treatment for biliary leak after pLT. Seven patients presented with leakage at the hepaticojejunostomy, two with leakage at the choledocho-choledochostomy and one with a bile leak because of an overlooked segmental bile duct. In terms of the mean, the PTBD treatment started 40.3 ± 31.7 days after pLT. The mean duration of PTBD treatment was 109.7 ± 103.6 days. Additional percutaneous bilioma drainage was required in eight cases. Bile leak treatment was successful in all cases, and no complications occurred. The patient and transplant survival rate was 100%. CRP serum level, leukocyte count, gamma-glutamyl transferase (GGT), and total and direct bilirubin level decreased significantly during treatment with a very strong effect size. Additionally, the gamma-glutamyl transferase level showed a statistically significant reduction during follow-up.
Conclusions: PTBD is a very successful strategy for bile leak therapy after pLT.
TomographyMedicine-Radiology, Nuclear Medicine and Imaging
CiteScore
2.70
自引率
10.50%
发文量
222
期刊介绍:
TomographyTM publishes basic (technical and pre-clinical) and clinical scientific articles which involve the advancement of imaging technologies. Tomography encompasses studies that use single or multiple imaging modalities including for example CT, US, PET, SPECT, MR and hyperpolarization technologies, as well as optical modalities (i.e. bioluminescence, photoacoustic, endomicroscopy, fiber optic imaging and optical computed tomography) in basic sciences, engineering, preclinical and clinical medicine.
Tomography also welcomes studies involving exploration and refinement of contrast mechanisms and image-derived metrics within and across modalities toward the development of novel imaging probes for image-based feedback and intervention. The use of imaging in biology and medicine provides unparalleled opportunities to noninvasively interrogate tissues to obtain real-time dynamic and quantitative information required for diagnosis and response to interventions and to follow evolving pathological conditions. As multi-modal studies and the complexities of imaging technologies themselves are ever increasing to provide advanced information to scientists and clinicians.
Tomography provides a unique publication venue allowing investigators the opportunity to more precisely communicate integrated findings related to the diverse and heterogeneous features associated with underlying anatomical, physiological, functional, metabolic and molecular genetic activities of normal and diseased tissue. Thus Tomography publishes peer-reviewed articles which involve the broad use of imaging of any tissue and disease type including both preclinical and clinical investigations. In addition, hardware/software along with chemical and molecular probe advances are welcome as they are deemed to significantly contribute towards the long-term goal of improving the overall impact of imaging on scientific and clinical discovery.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
