{"title":"采用平均机会成本和或有估值方法估算中国晚期癌症的成本效益阈值。","authors":"Qian Peng, Yue Yin, Min Liang, Mingye Zhao, Taihang Shao, Yaqian Tang, Zhiqing Mei, Hao Li, Wenxi Tang","doi":"10.1186/s12962-023-00487-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Monetizing health has sparked controversy and has implications for pricing strategies of emerging health technologies. Medical insurance payers typically set up thresholds for quality-adjusted life years (QALY) gains based on health productivity and budget affordability, but they rarely consider patient willingness-to-pay (WTP). Our study aims to compare Chinese payer threshold and patient WTP toward QALY gain of advanced non-small cell lung cancer (NSCLC) and to inform a potential inclusion of patient WTP under more complex decision-making scenarios.</p><p><strong>Methods: </strong>A regression model was constructed with cost as the independent variable and QALY as the dependent variable, where the regression coefficients reflect mean opportunity cost, and by transforming these coefficients, the payer threshold can be obtained. Patient WTP was elicited through a contingent valuation method survey. The robustness of the findings was examined through sensitivity analyses of model parameters and patient heterogeneity.</p><p><strong>Results: </strong>The payer mean threshold in the base-case was estimated at 150,962 yuan (1.86 times per capita GDP, 95% CI 144,041-159,204). The two scenarios analysis generated by different utility inputs yielded thresholds of 112,324 yuan (1.39 times per capita GDP) and 111,824 yuan (1.38 times per capita GDP), respectively. The survey included 85 patients, with a mean WTP of 148,443 yuan (1.83 times per capita GDP, 95% CI 120,994-175,893) and median value was 106,667 yuan (1.32 times the GDP per capita). Due to the substantial degree of dispersion, the median was more representative. The payer threshold was found to have a high probability (98.5%) of falling within the range of 1-2 times per capita GDP, while the robustness of patient WTP was relatively weak.</p><p><strong>Conclusions: </strong>In China, a country with a copayment system, payer threshold was higher than patient WTP, indicating that medical insurance holds significant decision-making authority, thus temporarily negating the need to consider patient WTP.</p>","PeriodicalId":47054,"journal":{"name":"Cost Effectiveness and Resource Allocation","volume":"21 1","pages":"80"},"PeriodicalIF":2.5000,"publicationDate":"2023-11-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10621116/pdf/","citationCount":"0","resultStr":"{\"title\":\"Estimating the cost-effectiveness threshold of advanced non-small cell lung cancer in China using mean opportunity cost and contingent valuation method.\",\"authors\":\"Qian Peng, Yue Yin, Min Liang, Mingye Zhao, Taihang Shao, Yaqian Tang, Zhiqing Mei, Hao Li, Wenxi Tang\",\"doi\":\"10.1186/s12962-023-00487-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Monetizing health has sparked controversy and has implications for pricing strategies of emerging health technologies. Medical insurance payers typically set up thresholds for quality-adjusted life years (QALY) gains based on health productivity and budget affordability, but they rarely consider patient willingness-to-pay (WTP). Our study aims to compare Chinese payer threshold and patient WTP toward QALY gain of advanced non-small cell lung cancer (NSCLC) and to inform a potential inclusion of patient WTP under more complex decision-making scenarios.</p><p><strong>Methods: </strong>A regression model was constructed with cost as the independent variable and QALY as the dependent variable, where the regression coefficients reflect mean opportunity cost, and by transforming these coefficients, the payer threshold can be obtained. Patient WTP was elicited through a contingent valuation method survey. The robustness of the findings was examined through sensitivity analyses of model parameters and patient heterogeneity.</p><p><strong>Results: </strong>The payer mean threshold in the base-case was estimated at 150,962 yuan (1.86 times per capita GDP, 95% CI 144,041-159,204). The two scenarios analysis generated by different utility inputs yielded thresholds of 112,324 yuan (1.39 times per capita GDP) and 111,824 yuan (1.38 times per capita GDP), respectively. The survey included 85 patients, with a mean WTP of 148,443 yuan (1.83 times per capita GDP, 95% CI 120,994-175,893) and median value was 106,667 yuan (1.32 times the GDP per capita). Due to the substantial degree of dispersion, the median was more representative. The payer threshold was found to have a high probability (98.5%) of falling within the range of 1-2 times per capita GDP, while the robustness of patient WTP was relatively weak.</p><p><strong>Conclusions: </strong>In China, a country with a copayment system, payer threshold was higher than patient WTP, indicating that medical insurance holds significant decision-making authority, thus temporarily negating the need to consider patient WTP.</p>\",\"PeriodicalId\":47054,\"journal\":{\"name\":\"Cost Effectiveness and Resource Allocation\",\"volume\":\"21 1\",\"pages\":\"80\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2023-11-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10621116/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cost Effectiveness and Resource Allocation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12962-023-00487-z\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH POLICY & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cost Effectiveness and Resource Allocation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12962-023-00487-z","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
Estimating the cost-effectiveness threshold of advanced non-small cell lung cancer in China using mean opportunity cost and contingent valuation method.
Objectives: Monetizing health has sparked controversy and has implications for pricing strategies of emerging health technologies. Medical insurance payers typically set up thresholds for quality-adjusted life years (QALY) gains based on health productivity and budget affordability, but they rarely consider patient willingness-to-pay (WTP). Our study aims to compare Chinese payer threshold and patient WTP toward QALY gain of advanced non-small cell lung cancer (NSCLC) and to inform a potential inclusion of patient WTP under more complex decision-making scenarios.
Methods: A regression model was constructed with cost as the independent variable and QALY as the dependent variable, where the regression coefficients reflect mean opportunity cost, and by transforming these coefficients, the payer threshold can be obtained. Patient WTP was elicited through a contingent valuation method survey. The robustness of the findings was examined through sensitivity analyses of model parameters and patient heterogeneity.
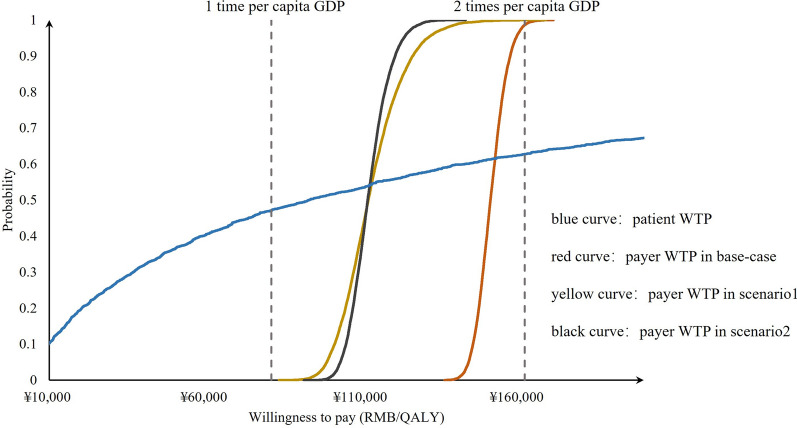
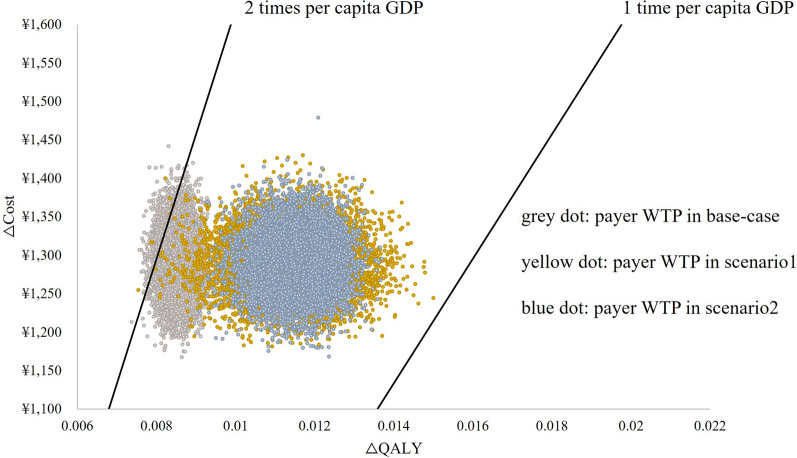
Results: The payer mean threshold in the base-case was estimated at 150,962 yuan (1.86 times per capita GDP, 95% CI 144,041-159,204). The two scenarios analysis generated by different utility inputs yielded thresholds of 112,324 yuan (1.39 times per capita GDP) and 111,824 yuan (1.38 times per capita GDP), respectively. The survey included 85 patients, with a mean WTP of 148,443 yuan (1.83 times per capita GDP, 95% CI 120,994-175,893) and median value was 106,667 yuan (1.32 times the GDP per capita). Due to the substantial degree of dispersion, the median was more representative. The payer threshold was found to have a high probability (98.5%) of falling within the range of 1-2 times per capita GDP, while the robustness of patient WTP was relatively weak.
Conclusions: In China, a country with a copayment system, payer threshold was higher than patient WTP, indicating that medical insurance holds significant decision-making authority, thus temporarily negating the need to consider patient WTP.
期刊介绍:
Cost Effectiveness and Resource Allocation is an Open Access, peer-reviewed, online journal that considers manuscripts on all aspects of cost-effectiveness analysis, including conceptual or methodological work, economic evaluations, and policy analysis related to resource allocation at a national or international level. Cost Effectiveness and Resource Allocation is aimed at health economists, health services researchers, and policy-makers with an interest in enhancing the flow and transfer of knowledge relating to efficiency in the health sector. Manuscripts are encouraged from researchers based in low- and middle-income countries, with a view to increasing the international economic evidence base for health.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
