Whitney A Perry, Jennifer K Chow, Jason Nelson, David M Kent, David R Snydman
{"title":"预测心脏移植术后第一年选择高危感染发生率的临床模型。","authors":"Whitney A Perry, Jennifer K Chow, Jason Nelson, David M Kent, David R Snydman","doi":"10.1097/TXD.0000000000001542","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Invasive infection remains a dangerous complication of heart transplantation (HT). No objectively defined set of clinical risk factors has been established to reliably predict infection in HT. The aim of this study was to develop a clinical prediction model for use at 1 mo post-HT to predict serious infection by 1 y.</p><p><strong>Methods: </strong>A retrospective cohort study of HT recipients (2000-2018) was performed. The composite endpoint included cytomegalovirus (CMV), herpes simplex or varicella zoster virus infection, blood stream infection, invasive fungal, or nocardial infection occurring 1 mo to 1 y post-HT. A least absolute shrinkage and selection operator regression model was constructed using 10 candidate variables. A concordance statistic, calibration curve, and mean calibration error were calculated. A scoring system was derived for ease of clinical application.</p><p><strong>Results: </strong>Three hundred seventy-five patients were analyzed; 93 patients experienced an outcome event. All variables remained in the final model: aged 55 y or above, history of diabetes, need for renal replacement therapy in first month, CMV risk derived from donor and recipient serology, use of induction and/or early lymphodepleting therapy in the first month, use of trimethoprim-sulfamethoxazole prophylaxis at 1 mo, lymphocyte count under 0.75 × 10<sup>3</sup>cells/µL at 1 mo, and inpatient status at 1 mo. Good discrimination (C-index 0.80) and calibration (mean absolute calibration error 3.6%) were demonstrated.</p><p><strong>Conclusion: </strong>This model synthesizes multiple highly relevant clinical parameters, available at 1 mo post-HT, into a unified, objective, and clinically useful prediction tool for occurrence of serious infection by 1 y post-HT.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"9 12","pages":"e1542"},"PeriodicalIF":1.9000,"publicationDate":"2023-11-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10624471/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Clinical Model to Predict the Occurrence of Select High-risk Infections in the First Year Following Heart Transplantation.\",\"authors\":\"Whitney A Perry, Jennifer K Chow, Jason Nelson, David M Kent, David R Snydman\",\"doi\":\"10.1097/TXD.0000000000001542\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Invasive infection remains a dangerous complication of heart transplantation (HT). No objectively defined set of clinical risk factors has been established to reliably predict infection in HT. The aim of this study was to develop a clinical prediction model for use at 1 mo post-HT to predict serious infection by 1 y.</p><p><strong>Methods: </strong>A retrospective cohort study of HT recipients (2000-2018) was performed. The composite endpoint included cytomegalovirus (CMV), herpes simplex or varicella zoster virus infection, blood stream infection, invasive fungal, or nocardial infection occurring 1 mo to 1 y post-HT. A least absolute shrinkage and selection operator regression model was constructed using 10 candidate variables. A concordance statistic, calibration curve, and mean calibration error were calculated. A scoring system was derived for ease of clinical application.</p><p><strong>Results: </strong>Three hundred seventy-five patients were analyzed; 93 patients experienced an outcome event. All variables remained in the final model: aged 55 y or above, history of diabetes, need for renal replacement therapy in first month, CMV risk derived from donor and recipient serology, use of induction and/or early lymphodepleting therapy in the first month, use of trimethoprim-sulfamethoxazole prophylaxis at 1 mo, lymphocyte count under 0.75 × 10<sup>3</sup>cells/µL at 1 mo, and inpatient status at 1 mo. Good discrimination (C-index 0.80) and calibration (mean absolute calibration error 3.6%) were demonstrated.</p><p><strong>Conclusion: </strong>This model synthesizes multiple highly relevant clinical parameters, available at 1 mo post-HT, into a unified, objective, and clinically useful prediction tool for occurrence of serious infection by 1 y post-HT.</p>\",\"PeriodicalId\":23225,\"journal\":{\"name\":\"Transplantation Direct\",\"volume\":\"9 12\",\"pages\":\"e1542\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2023-11-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10624471/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplantation Direct\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/TXD.0000000000001542\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/12/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"TRANSPLANTATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001542","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
A Clinical Model to Predict the Occurrence of Select High-risk Infections in the First Year Following Heart Transplantation.
Background: Invasive infection remains a dangerous complication of heart transplantation (HT). No objectively defined set of clinical risk factors has been established to reliably predict infection in HT. The aim of this study was to develop a clinical prediction model for use at 1 mo post-HT to predict serious infection by 1 y.
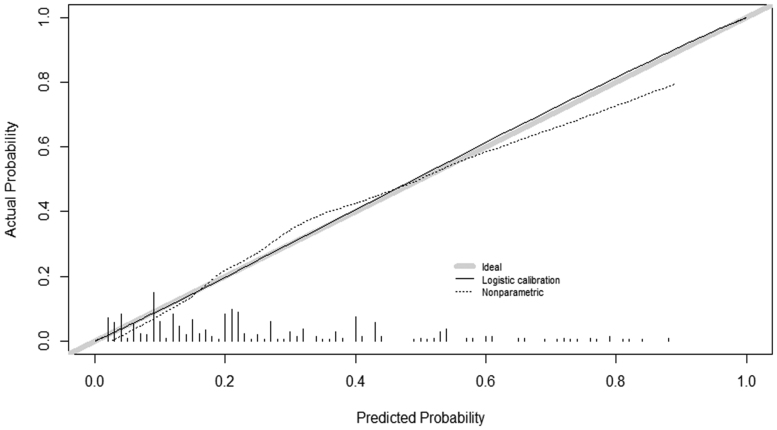
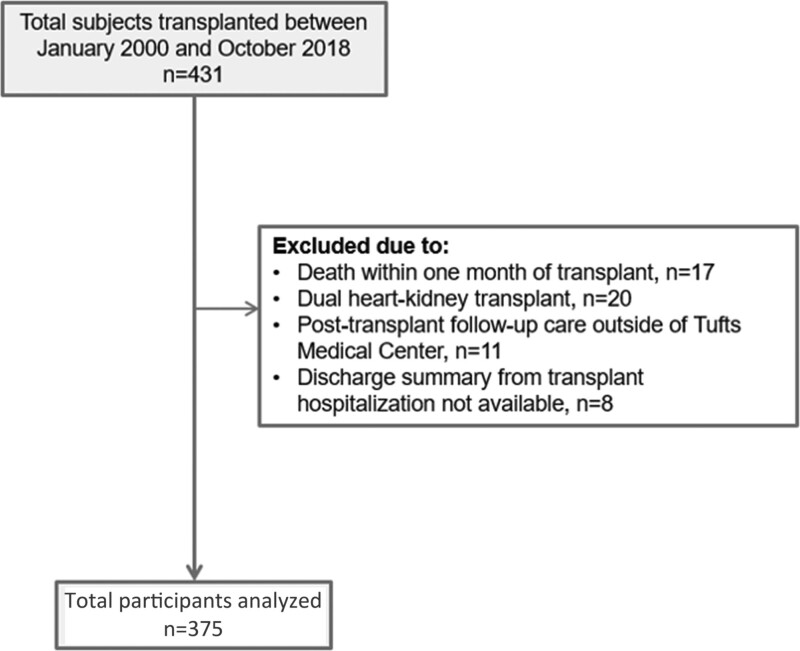
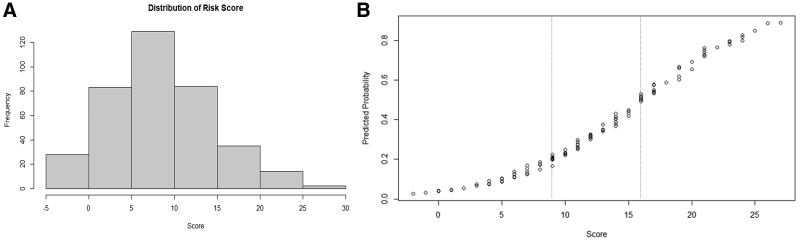
Methods: A retrospective cohort study of HT recipients (2000-2018) was performed. The composite endpoint included cytomegalovirus (CMV), herpes simplex or varicella zoster virus infection, blood stream infection, invasive fungal, or nocardial infection occurring 1 mo to 1 y post-HT. A least absolute shrinkage and selection operator regression model was constructed using 10 candidate variables. A concordance statistic, calibration curve, and mean calibration error were calculated. A scoring system was derived for ease of clinical application.
Results: Three hundred seventy-five patients were analyzed; 93 patients experienced an outcome event. All variables remained in the final model: aged 55 y or above, history of diabetes, need for renal replacement therapy in first month, CMV risk derived from donor and recipient serology, use of induction and/or early lymphodepleting therapy in the first month, use of trimethoprim-sulfamethoxazole prophylaxis at 1 mo, lymphocyte count under 0.75 × 103cells/µL at 1 mo, and inpatient status at 1 mo. Good discrimination (C-index 0.80) and calibration (mean absolute calibration error 3.6%) were demonstrated.
Conclusion: This model synthesizes multiple highly relevant clinical parameters, available at 1 mo post-HT, into a unified, objective, and clinically useful prediction tool for occurrence of serious infection by 1 y post-HT.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
