Ciro Celsa, Giuseppe Cabibbo, David James Pinato, Gabriele Di Maria, Marco Enea, Marco Vaccaro, Salvatore Battaglia, Giacomo Emanuele Maria Rizzo, Paolo Giuffrida, Carmelo Marco Giacchetto, Gabriele Rancatore, Maria Vittoria Grassini, Calogero Cammà
{"title":"平衡晚期肝细胞癌一线系统疗法的疗效和耐受性:一项网络 Meta 分析。","authors":"Ciro Celsa, Giuseppe Cabibbo, David James Pinato, Gabriele Di Maria, Marco Enea, Marco Vaccaro, Salvatore Battaglia, Giacomo Emanuele Maria Rizzo, Paolo Giuffrida, Carmelo Marco Giacchetto, Gabriele Rancatore, Maria Vittoria Grassini, Calogero Cammà","doi":"10.1159/000531744","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Atezolizumab + bevacizumab represent the current standard of care for first-line treatment of advanced hepatocellular carcinoma (HCC). However, direct comparison with other combination treatments including immune checkpoint inhibitors (ICI) + tyrosine kinase inhibitors (TKIs) are lacking.</p><p><strong>Objectives: </strong>This network meta-analysis (NMA) aims to indirectly compare the efficacy and the safety of first-line systemic therapies for unresectable advanced HCC.</p><p><strong>Method: </strong>A literature search of MEDLINE, Embase, and SCOPUS databases was conducted up to October 31, 2022. Phase 3 randomized controlled trials (RCTs) testing TKIs, including sorafenib and lenvatinib, or ICIs reporting overall survival (OS) and progression-free survival (PFS) were included. Individual survival data were extracted from OS and PFS curves to calculate restricted mean survival time. A Bayesian NMA was performed to compare treatments in terms of efficacy (15- and 30-month OS, 6-month PFS) and safety, represented by grade ≥3 (severe) adverse events (SAEs). The incremental safety-effectiveness ratio as measure of net health benefit was calculated as the difference in SAE probability divided by survival difference between the 2 most effective treatments.</p><p><strong>Results: </strong>Nine RCTs enrolling 6,600 patients were included. Atezolizumab plus bevacizumab showed the highest probability (88%) of achieving the 30-month OS landmark. Lenvatinib showed a probability of 86% of achieving best PFS outcomes. ICI monotherapies ranked as most tolerable. Atezolizumab plus bevacizumab showed the best net health benefit for OS, compared to durvalumab plus tremelimumab. When evaluating the net health benefit for PFS, at a willingness-to-risk threshold of 10% of SAEs for life-month gained, atezolizumab plus bevacizumab was favoured in 78% of cases, while at threshold of 30% of SAEs for life-month gained, lenvatinib was favoured in 76% of cases.</p><p><strong>Conclusions: </strong>Atezolizumab plus bevacizumab is the best treatment in terms of net benefit and therefore it should be recommended as standard of care. Compared to atezolizumab plus bevacizumab, lenvatinib monotherapy had the best net benefit for PFS when physicians and patients are available to accept a higher risk of toxicity.</p>","PeriodicalId":50285,"journal":{"name":"International Journal of Technology Management","volume":"1 1","pages":"169-180"},"PeriodicalIF":1.4000,"publicationDate":"2023-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11095611/pdf/","citationCount":"0","resultStr":"{\"title\":\"Balancing Efficacy and Tolerability of First-Line Systemic Therapies for Advanced Hepatocellular Carcinoma: A Network Meta-Analysis.\",\"authors\":\"Ciro Celsa, Giuseppe Cabibbo, David James Pinato, Gabriele Di Maria, Marco Enea, Marco Vaccaro, Salvatore Battaglia, Giacomo Emanuele Maria Rizzo, Paolo Giuffrida, Carmelo Marco Giacchetto, Gabriele Rancatore, Maria Vittoria Grassini, Calogero Cammà\",\"doi\":\"10.1159/000531744\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Atezolizumab + bevacizumab represent the current standard of care for first-line treatment of advanced hepatocellular carcinoma (HCC). However, direct comparison with other combination treatments including immune checkpoint inhibitors (ICI) + tyrosine kinase inhibitors (TKIs) are lacking.</p><p><strong>Objectives: </strong>This network meta-analysis (NMA) aims to indirectly compare the efficacy and the safety of first-line systemic therapies for unresectable advanced HCC.</p><p><strong>Method: </strong>A literature search of MEDLINE, Embase, and SCOPUS databases was conducted up to October 31, 2022. Phase 3 randomized controlled trials (RCTs) testing TKIs, including sorafenib and lenvatinib, or ICIs reporting overall survival (OS) and progression-free survival (PFS) were included. Individual survival data were extracted from OS and PFS curves to calculate restricted mean survival time. A Bayesian NMA was performed to compare treatments in terms of efficacy (15- and 30-month OS, 6-month PFS) and safety, represented by grade ≥3 (severe) adverse events (SAEs). The incremental safety-effectiveness ratio as measure of net health benefit was calculated as the difference in SAE probability divided by survival difference between the 2 most effective treatments.</p><p><strong>Results: </strong>Nine RCTs enrolling 6,600 patients were included. Atezolizumab plus bevacizumab showed the highest probability (88%) of achieving the 30-month OS landmark. Lenvatinib showed a probability of 86% of achieving best PFS outcomes. ICI monotherapies ranked as most tolerable. Atezolizumab plus bevacizumab showed the best net health benefit for OS, compared to durvalumab plus tremelimumab. When evaluating the net health benefit for PFS, at a willingness-to-risk threshold of 10% of SAEs for life-month gained, atezolizumab plus bevacizumab was favoured in 78% of cases, while at threshold of 30% of SAEs for life-month gained, lenvatinib was favoured in 76% of cases.</p><p><strong>Conclusions: </strong>Atezolizumab plus bevacizumab is the best treatment in terms of net benefit and therefore it should be recommended as standard of care. Compared to atezolizumab plus bevacizumab, lenvatinib monotherapy had the best net benefit for PFS when physicians and patients are available to accept a higher risk of toxicity.</p>\",\"PeriodicalId\":50285,\"journal\":{\"name\":\"International Journal of Technology Management\",\"volume\":\"1 1\",\"pages\":\"169-180\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2023-07-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11095611/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Technology Management\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1159/000531744\",\"RegionNum\":4,\"RegionCategory\":\"管理学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ENGINEERING, MULTIDISCIPLINARY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Technology Management","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000531744","RegionNum":4,"RegionCategory":"管理学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/4/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENGINEERING, MULTIDISCIPLINARY","Score":null,"Total":0}
Balancing Efficacy and Tolerability of First-Line Systemic Therapies for Advanced Hepatocellular Carcinoma: A Network Meta-Analysis.
Background: Atezolizumab + bevacizumab represent the current standard of care for first-line treatment of advanced hepatocellular carcinoma (HCC). However, direct comparison with other combination treatments including immune checkpoint inhibitors (ICI) + tyrosine kinase inhibitors (TKIs) are lacking.
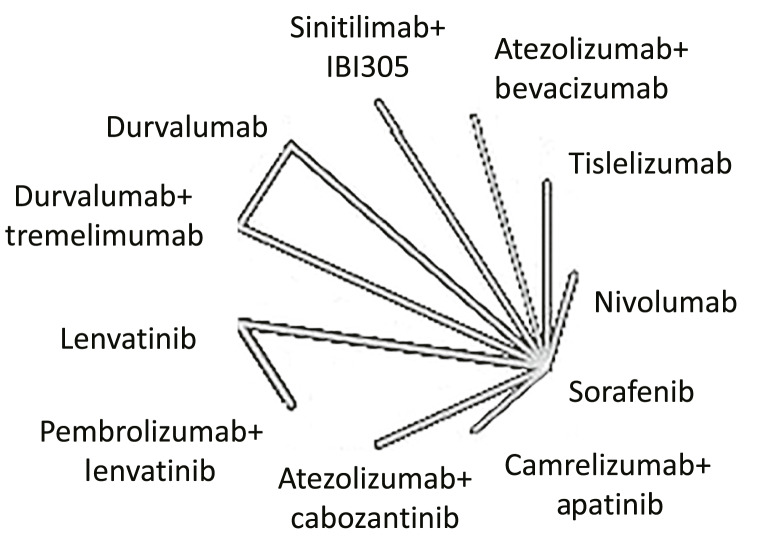
Objectives: This network meta-analysis (NMA) aims to indirectly compare the efficacy and the safety of first-line systemic therapies for unresectable advanced HCC.
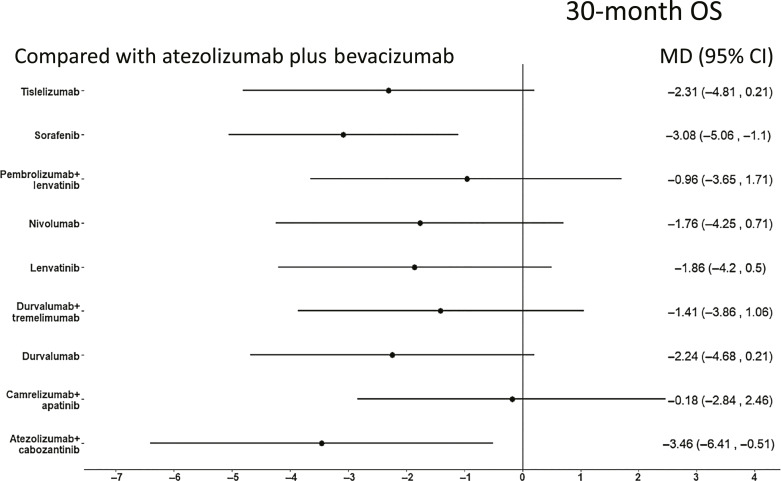
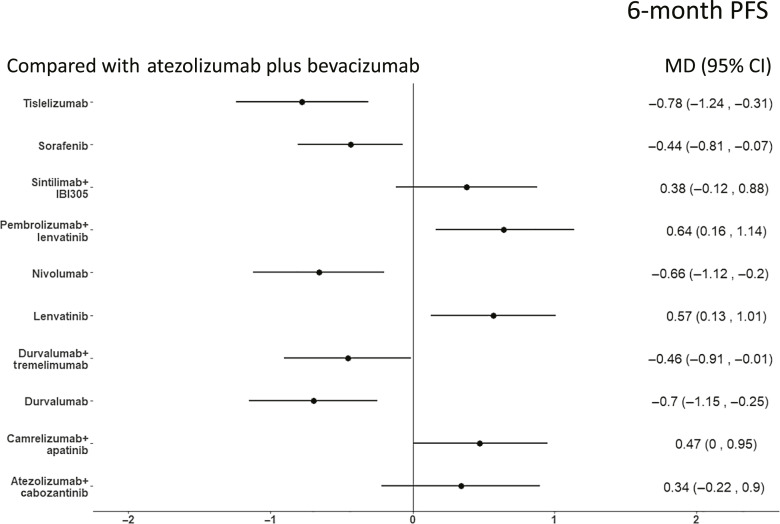
Method: A literature search of MEDLINE, Embase, and SCOPUS databases was conducted up to October 31, 2022. Phase 3 randomized controlled trials (RCTs) testing TKIs, including sorafenib and lenvatinib, or ICIs reporting overall survival (OS) and progression-free survival (PFS) were included. Individual survival data were extracted from OS and PFS curves to calculate restricted mean survival time. A Bayesian NMA was performed to compare treatments in terms of efficacy (15- and 30-month OS, 6-month PFS) and safety, represented by grade ≥3 (severe) adverse events (SAEs). The incremental safety-effectiveness ratio as measure of net health benefit was calculated as the difference in SAE probability divided by survival difference between the 2 most effective treatments.
Results: Nine RCTs enrolling 6,600 patients were included. Atezolizumab plus bevacizumab showed the highest probability (88%) of achieving the 30-month OS landmark. Lenvatinib showed a probability of 86% of achieving best PFS outcomes. ICI monotherapies ranked as most tolerable. Atezolizumab plus bevacizumab showed the best net health benefit for OS, compared to durvalumab plus tremelimumab. When evaluating the net health benefit for PFS, at a willingness-to-risk threshold of 10% of SAEs for life-month gained, atezolizumab plus bevacizumab was favoured in 78% of cases, while at threshold of 30% of SAEs for life-month gained, lenvatinib was favoured in 76% of cases.
Conclusions: Atezolizumab plus bevacizumab is the best treatment in terms of net benefit and therefore it should be recommended as standard of care. Compared to atezolizumab plus bevacizumab, lenvatinib monotherapy had the best net benefit for PFS when physicians and patients are available to accept a higher risk of toxicity.
期刊介绍:
The IJTM aims to provide a refereed and authoritative source of information in the field of managing with technology, and the management of engineering, science and technology. It seeks to establish channels of communication between government departments, technology executives in industry, commerce and related business, and academic experts in the field.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
