Kemei Zhang, Shisi Huang, Haiyan Xu, Jiaou Zhang, Ensheng Wang, Yang Li, Changling Zhu, Jing Shu
{"title":"促性腺激素释放激素激动剂疗法改善 I-II 期子宫内膜异位症患者宫腔内人工授精效果的有效性。","authors":"Kemei Zhang, Shisi Huang, Haiyan Xu, Jiaou Zhang, Ensheng Wang, Yang Li, Changling Zhu, Jing Shu","doi":"10.1080/07853890.2022.2071458","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To explore the role of postoperative gonadotrophin releasing hormone agonist (GnRH-a) therapy before treatment with intrauterine insemination (IUI) for infertile females with stage I-II endometriosis.</p><p><strong>Material and methods: </strong>Ninety-seven patients diagnosed with stage I-II endometriosis before IUI were enrolled in this study. The clinical pregnancy rate, cumulative pregnancy rate, live birth rate and newborn conditions were compared between the two groups with and without GnRH-a therapy.</p><p><strong>Results: </strong>The clinical pregnancy rate of IUI in the GnRH-a group was higher than that in the control group (15.29% vs. 11.82%, <i>p</i> = .035). By logistic regression analysis, patients treated with GnRH-a had a higher clinical pregnancy rate than those without (adjusted odds ratio (AOR) 23.190, 95% confidence interval (CI) 1.238-434.312). The live birth rate per IUI cycle in the GnRH-a group was also higher than in the controls (12.94% vs. 10%). However, the difference was not statistically significant (<i>p</i> = .311, AOR 4.844, 95% CI 0.229-102.320). The patients with GnRH-a therapy had a similar incidence of multiple pregnancy rate (0% vs. 0%), miscarriage rate (2.35% vs. 0.91%) and ectopic pregnancy rate (0% vs. 0.91%) as compared to the control group. The cumulative pregnancy rates were all higher in patients administered with GnRH-a than those without GnRH-a treatment in different cycles (one cycle: 17.07% vs 12.50%; two cycles: 29.27% vs 19.64%; three cycles: 31.71% vs 23.21%; ≥four cycles: 31.71% vs 23.21%), but the difference was not statistically significant. Notably, there was no more pregnancy after the third IUI cycle. The gestation weeks of delivery in the two groups were 39.09 ± 1.04 and 38.60 ± 1.17, respectively (<i>p</i> = .323). Nor was there difference in birth weight between the two groups (3236 ± 537 g vs 3435 ± 418 g, <i>p</i> = .360).</p><p><strong>Conclusions: </strong>The administration of GnRH-a in patients with stage I-II endometriosis could be beneficial to the outcomes of IUI. It is recommended that IUI should be discontinued after three failed attempts. KEY MESSAGESEndometriosis is a common cause of infertility, but the exact mechanism remains unclear.The administration of GnRH-a before IUI treatment is beneficial for patients suffering from stage I-II endometriosis.After three failed attempts, IUI should be stopped in patients with stage I-II endometriosis.</p>","PeriodicalId":46532,"journal":{"name":"Journal of the Philosophy of Sport","volume":"34 1","pages":"1330-1338"},"PeriodicalIF":1.7000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9126587/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effectiveness of gonadotrophin-releasing hormone agonist therapy to improve the outcomes of intrauterine insemination in patients suffering from stage I-II endometriosis.\",\"authors\":\"Kemei Zhang, Shisi Huang, Haiyan Xu, Jiaou Zhang, Ensheng Wang, Yang Li, Changling Zhu, Jing Shu\",\"doi\":\"10.1080/07853890.2022.2071458\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To explore the role of postoperative gonadotrophin releasing hormone agonist (GnRH-a) therapy before treatment with intrauterine insemination (IUI) for infertile females with stage I-II endometriosis.</p><p><strong>Material and methods: </strong>Ninety-seven patients diagnosed with stage I-II endometriosis before IUI were enrolled in this study. The clinical pregnancy rate, cumulative pregnancy rate, live birth rate and newborn conditions were compared between the two groups with and without GnRH-a therapy.</p><p><strong>Results: </strong>The clinical pregnancy rate of IUI in the GnRH-a group was higher than that in the control group (15.29% vs. 11.82%, <i>p</i> = .035). By logistic regression analysis, patients treated with GnRH-a had a higher clinical pregnancy rate than those without (adjusted odds ratio (AOR) 23.190, 95% confidence interval (CI) 1.238-434.312). The live birth rate per IUI cycle in the GnRH-a group was also higher than in the controls (12.94% vs. 10%). However, the difference was not statistically significant (<i>p</i> = .311, AOR 4.844, 95% CI 0.229-102.320). The patients with GnRH-a therapy had a similar incidence of multiple pregnancy rate (0% vs. 0%), miscarriage rate (2.35% vs. 0.91%) and ectopic pregnancy rate (0% vs. 0.91%) as compared to the control group. The cumulative pregnancy rates were all higher in patients administered with GnRH-a than those without GnRH-a treatment in different cycles (one cycle: 17.07% vs 12.50%; two cycles: 29.27% vs 19.64%; three cycles: 31.71% vs 23.21%; ≥four cycles: 31.71% vs 23.21%), but the difference was not statistically significant. Notably, there was no more pregnancy after the third IUI cycle. The gestation weeks of delivery in the two groups were 39.09 ± 1.04 and 38.60 ± 1.17, respectively (<i>p</i> = .323). Nor was there difference in birth weight between the two groups (3236 ± 537 g vs 3435 ± 418 g, <i>p</i> = .360).</p><p><strong>Conclusions: </strong>The administration of GnRH-a in patients with stage I-II endometriosis could be beneficial to the outcomes of IUI. It is recommended that IUI should be discontinued after three failed attempts. KEY MESSAGESEndometriosis is a common cause of infertility, but the exact mechanism remains unclear.The administration of GnRH-a before IUI treatment is beneficial for patients suffering from stage I-II endometriosis.After three failed attempts, IUI should be stopped in patients with stage I-II endometriosis.</p>\",\"PeriodicalId\":46532,\"journal\":{\"name\":\"Journal of the Philosophy of Sport\",\"volume\":\"34 1\",\"pages\":\"1330-1338\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9126587/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Philosophy of Sport\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1080/07853890.2022.2071458\",\"RegionNum\":3,\"RegionCategory\":\"哲学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ETHICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Philosophy of Sport","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1080/07853890.2022.2071458","RegionNum":3,"RegionCategory":"哲学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ETHICS","Score":null,"Total":0}
引用次数: 0
摘要
目的探讨子宫内膜异位症I-II期不孕女性在接受宫腔内人工授精(IUI)治疗前术后使用促性腺激素释放激素激动剂(GnRH-a)治疗的作用:本研究共纳入了97例在宫腔内人工授精前确诊为I-II期子宫内膜异位症的患者。比较两组接受和未接受 GnRH-a 治疗的患者的临床妊娠率、累积妊娠率、活产率和新生儿情况:结果:GnRH-a 组人工授精的临床妊娠率高于对照组(15.29% 对 11.82%,P = 0.035)。通过逻辑回归分析,接受 GnRH-a 治疗的患者的临床妊娠率高于未接受 GnRH-a 治疗的患者(调整后的几率比(AOR)为 23.190,95% 置信区间(CI)为 1.238-434.312)。GnRH-a 组每个人工授精周期的活产率也高于对照组(12.94% 对 10%)。然而,差异并无统计学意义(P = .311,AOR 4.844,95% CI 0.229-102.320)。与对照组相比,接受 GnRH-a 治疗的患者多胎妊娠率(0% vs. 0%)、流产率(2.35% vs. 0.91%)和宫外孕率(0% vs. 0.91%)的发生率相似。使用 GnRH-a 的患者在不同周期的累积妊娠率均高于未使用 GnRH-a 的患者(一个周期:17.07% vs 12.50%;两个周期:29.27% vs 19.64%):29.27% vs 19.64%;三个周期:31.71% vs 23.21%):31.71% vs 23.21%;≥四个周期:31.71% vs 23.21%),但差异无统计学意义。值得注意的是,第三个人工授精周期后没有再怀孕。两组的分娩孕周分别为(39.09 ± 1.04)和(38.60 ± 1.17)(P = 0.323)。两组的出生体重也没有差异(3236 ± 537 g vs 3435 ± 418 g,p = .360):结论:对 I-II 期子宫内膜异位症患者施用 GnRH-a 可能有利于人工授精的效果。结论:对 I-II 期子宫内膜异位症患者施用 GnRH-a 有益,但建议在三次尝试失败后停止人工授精。关键信息:子宫内膜异位症是导致不孕的常见原因,但其确切机制仍不清楚。在人工授精治疗前使用 GnRH-a 对 I-II 期子宫内膜异位症患者有益。
Effectiveness of gonadotrophin-releasing hormone agonist therapy to improve the outcomes of intrauterine insemination in patients suffering from stage I-II endometriosis.
Objective: To explore the role of postoperative gonadotrophin releasing hormone agonist (GnRH-a) therapy before treatment with intrauterine insemination (IUI) for infertile females with stage I-II endometriosis.
Material and methods: Ninety-seven patients diagnosed with stage I-II endometriosis before IUI were enrolled in this study. The clinical pregnancy rate, cumulative pregnancy rate, live birth rate and newborn conditions were compared between the two groups with and without GnRH-a therapy.
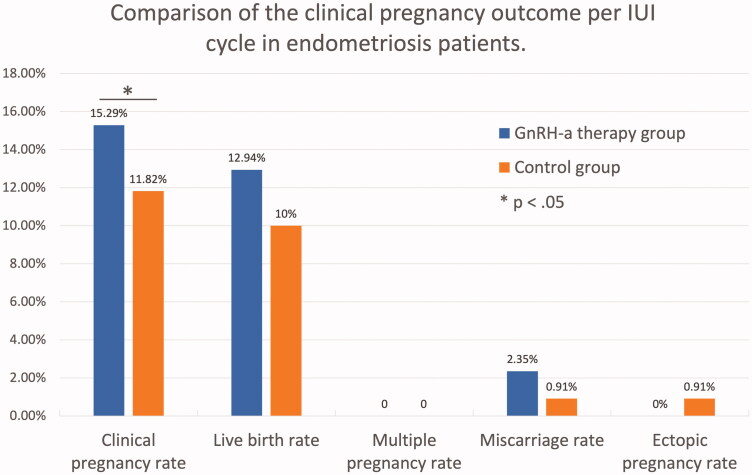
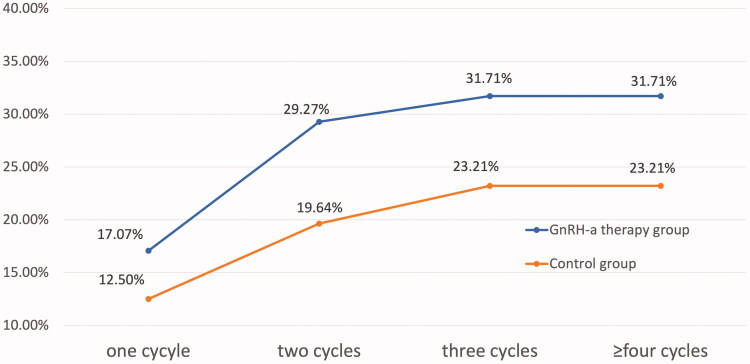
Results: The clinical pregnancy rate of IUI in the GnRH-a group was higher than that in the control group (15.29% vs. 11.82%, p = .035). By logistic regression analysis, patients treated with GnRH-a had a higher clinical pregnancy rate than those without (adjusted odds ratio (AOR) 23.190, 95% confidence interval (CI) 1.238-434.312). The live birth rate per IUI cycle in the GnRH-a group was also higher than in the controls (12.94% vs. 10%). However, the difference was not statistically significant (p = .311, AOR 4.844, 95% CI 0.229-102.320). The patients with GnRH-a therapy had a similar incidence of multiple pregnancy rate (0% vs. 0%), miscarriage rate (2.35% vs. 0.91%) and ectopic pregnancy rate (0% vs. 0.91%) as compared to the control group. The cumulative pregnancy rates were all higher in patients administered with GnRH-a than those without GnRH-a treatment in different cycles (one cycle: 17.07% vs 12.50%; two cycles: 29.27% vs 19.64%; three cycles: 31.71% vs 23.21%; ≥four cycles: 31.71% vs 23.21%), but the difference was not statistically significant. Notably, there was no more pregnancy after the third IUI cycle. The gestation weeks of delivery in the two groups were 39.09 ± 1.04 and 38.60 ± 1.17, respectively (p = .323). Nor was there difference in birth weight between the two groups (3236 ± 537 g vs 3435 ± 418 g, p = .360).
Conclusions: The administration of GnRH-a in patients with stage I-II endometriosis could be beneficial to the outcomes of IUI. It is recommended that IUI should be discontinued after three failed attempts. KEY MESSAGESEndometriosis is a common cause of infertility, but the exact mechanism remains unclear.The administration of GnRH-a before IUI treatment is beneficial for patients suffering from stage I-II endometriosis.After three failed attempts, IUI should be stopped in patients with stage I-II endometriosis.
期刊介绍:
The Journal of the Philosophy of Sport (JPS) is the most respected medium for communicating contemporary philosophic thought with regard to sport. It contains stimulating articles, critical reviews of work completed, and philosophic discussions about the philosophy of sport. JPS is published twice a year for the International Association for the Philosophy of Sport; members receive it as part of their membership. To subscribe to either the print or e-version of JPS, press the Subscribe or Renew button at the top of this screen.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
