{"title":"美国商业保险晚期或复发子宫内膜癌患者开始一线治疗的医疗资源利用和成本","authors":"Monica Kobayashi, Jamie Garside, Joehl Nguyen","doi":"10.36469/001c.88419","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Endometrial cancer (EC) represents a substantial economic burden for patients in the United States. Patients with advanced or recurrent EC have a much poorer prognosis than patients with early-stage EC. Data on healthcare resource utilization (HCRU) and costs for patients with advanced or recurrent EC specifically are lacking. <b>Objectives:</b> To describe HCRU and costs associated with first-line (1L) therapy for commercially insured patients with advanced or recurrent EC in the United States. <b>Methods:</b> This was a retrospective cohort study of adult patients with advanced or recurrent EC using the MarketScan® database. Treatment characteristics, HCRU, and costs were assessed from the first claim in the patient record for 1L therapy for advanced or recurrent EC (index) until initiation of a new anti-cancer therapy, disenrollment from the database, or the end of data availability. Baseline demographics were determined during the 12 months before the patient's index date. <b>Results:</b> A total of 7932 patients were eligible for inclusion. Overall, mean age at index was 61 years, most patients (77.3%) had received prior surgery for EC, and the most common 1L regimen was carboplatin/paclitaxel (59.1%). During the observation period, most patients had at least one healthcare visit (all-cause, 99.9%; EC-related, 82.8%), most commonly outpatient visits (all-cause, 91.4%; EC-related, 68.7%). The highest mean (SD) costs (US dollars) were for inpatient hospitalization for both all-cause and EC-related events ($8396 [$15,130] and $9436 [$16,784], respectively). Total costs were higher for patients with a diagnosis of metastasis at baseline than for those without a diagnosis of metastasis. <b>Discussion:</b> For patients with advanced or recurrent EC in the United States, 1L therapy is associated with considerable HCRU and economic burden. They are particularly high for patients with metastatic disease. <b>Conclusions:</b> This study highlights the need for new cost-effective treatments for patients with newly diagnosed advanced or recurrent EC.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"10 2","pages":"104-110"},"PeriodicalIF":2.5000,"publicationDate":"2023-11-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10637624/pdf/","citationCount":"0","resultStr":"{\"title\":\"Healthcare Resource Utilization and Costs Among Commercially Insured Patients With Advanced or Recurrent Endometrial Cancer Initiating First-Line Therapy in the United States.\",\"authors\":\"Monica Kobayashi, Jamie Garside, Joehl Nguyen\",\"doi\":\"10.36469/001c.88419\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> Endometrial cancer (EC) represents a substantial economic burden for patients in the United States. Patients with advanced or recurrent EC have a much poorer prognosis than patients with early-stage EC. Data on healthcare resource utilization (HCRU) and costs for patients with advanced or recurrent EC specifically are lacking. <b>Objectives:</b> To describe HCRU and costs associated with first-line (1L) therapy for commercially insured patients with advanced or recurrent EC in the United States. <b>Methods:</b> This was a retrospective cohort study of adult patients with advanced or recurrent EC using the MarketScan® database. Treatment characteristics, HCRU, and costs were assessed from the first claim in the patient record for 1L therapy for advanced or recurrent EC (index) until initiation of a new anti-cancer therapy, disenrollment from the database, or the end of data availability. Baseline demographics were determined during the 12 months before the patient's index date. <b>Results:</b> A total of 7932 patients were eligible for inclusion. Overall, mean age at index was 61 years, most patients (77.3%) had received prior surgery for EC, and the most common 1L regimen was carboplatin/paclitaxel (59.1%). During the observation period, most patients had at least one healthcare visit (all-cause, 99.9%; EC-related, 82.8%), most commonly outpatient visits (all-cause, 91.4%; EC-related, 68.7%). The highest mean (SD) costs (US dollars) were for inpatient hospitalization for both all-cause and EC-related events ($8396 [$15,130] and $9436 [$16,784], respectively). Total costs were higher for patients with a diagnosis of metastasis at baseline than for those without a diagnosis of metastasis. <b>Discussion:</b> For patients with advanced or recurrent EC in the United States, 1L therapy is associated with considerable HCRU and economic burden. They are particularly high for patients with metastatic disease. <b>Conclusions:</b> This study highlights the need for new cost-effective treatments for patients with newly diagnosed advanced or recurrent EC.</p>\",\"PeriodicalId\":16012,\"journal\":{\"name\":\"Journal of Health Economics and Outcomes Research\",\"volume\":\"10 2\",\"pages\":\"104-110\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2023-11-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10637624/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Health Economics and Outcomes Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.36469/001c.88419\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.88419","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
Healthcare Resource Utilization and Costs Among Commercially Insured Patients With Advanced or Recurrent Endometrial Cancer Initiating First-Line Therapy in the United States.
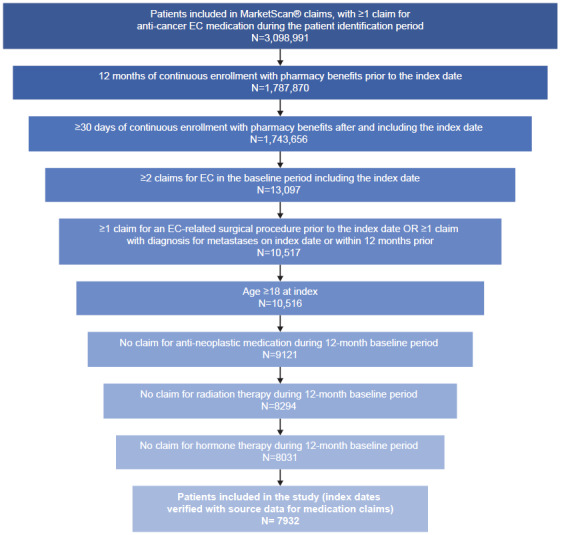
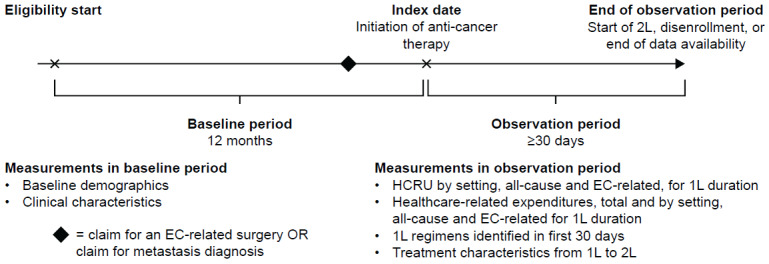
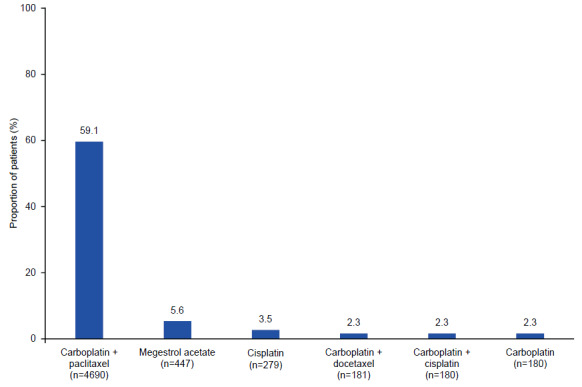
Background: Endometrial cancer (EC) represents a substantial economic burden for patients in the United States. Patients with advanced or recurrent EC have a much poorer prognosis than patients with early-stage EC. Data on healthcare resource utilization (HCRU) and costs for patients with advanced or recurrent EC specifically are lacking. Objectives: To describe HCRU and costs associated with first-line (1L) therapy for commercially insured patients with advanced or recurrent EC in the United States. Methods: This was a retrospective cohort study of adult patients with advanced or recurrent EC using the MarketScan® database. Treatment characteristics, HCRU, and costs were assessed from the first claim in the patient record for 1L therapy for advanced or recurrent EC (index) until initiation of a new anti-cancer therapy, disenrollment from the database, or the end of data availability. Baseline demographics were determined during the 12 months before the patient's index date. Results: A total of 7932 patients were eligible for inclusion. Overall, mean age at index was 61 years, most patients (77.3%) had received prior surgery for EC, and the most common 1L regimen was carboplatin/paclitaxel (59.1%). During the observation period, most patients had at least one healthcare visit (all-cause, 99.9%; EC-related, 82.8%), most commonly outpatient visits (all-cause, 91.4%; EC-related, 68.7%). The highest mean (SD) costs (US dollars) were for inpatient hospitalization for both all-cause and EC-related events ($8396 [$15,130] and $9436 [$16,784], respectively). Total costs were higher for patients with a diagnosis of metastasis at baseline than for those without a diagnosis of metastasis. Discussion: For patients with advanced or recurrent EC in the United States, 1L therapy is associated with considerable HCRU and economic burden. They are particularly high for patients with metastatic disease. Conclusions: This study highlights the need for new cost-effective treatments for patients with newly diagnosed advanced or recurrent EC.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
