Lewei Duan, Ming-Sum Lee, Jason N Doctor, John L Adams
{"title":"用先验知识引导方法解决未测量的混杂偏倚:稳定缺血性心脏病患者冠状动脉旁路移植术(CABG)与经皮冠状动脉介入治疗(PCI)","authors":"Lewei Duan, Ming-Sum Lee, Jason N Doctor, John L Adams","doi":"10.1007/s10742-022-00282-y","DOIUrl":null,"url":null,"abstract":"<p><p>Unmeasured confounding undermines the validity of observational studies. Although randomized clinical trials (RCTs) are considered the \"gold standard\" of study types, we often observe divergent findings between RCTs and empirical settings. We present the \"L-table\", a simulation-based, prior knowledge (e.g., RCTs) guided approach that estimates the true effect adjusting for the potential influence of unmeasured confounders when using observational data. Using electronic health record data from Kaiser Permanente Southern California, we compare the effectiveness of coronary artery bypass grafting (CABG) and percutaneous coronary intervention (PCI) on endpoints at 1, 3, 5, and 10 years for patients with stable ischemic heart disease. We applied the L-table approach to the propensity score adjusted cohort to derive the omitted-confounder-adjusted estimated effects. After the L-table adjustment, CABG patients are 57.6% less likely to encounter major adverse cardiac and cerebrovascular event (MACCE) at 1 year (OR [95% CI] 0.424 [0.396, 0.517]), 56.4% less likely at 3 years (OR [95% CI] 0.436 [0.369, 0.527]), and 48.9% less likely at 5 years (OR [95% CI] 0.511 [0.451, 0.538]). CABG patients are also 49.5% less likely to die by the end of 10 years than PCI patients (OR [95% CI] 0.505 [0.446, 0.582]). We found the estimated true effects all shifted towards CABG as a more effective procedure that led to better health outcomes compared to PCI. Unlike existing sensitivity tools, the L-table approach explicitly lays out probable values and can therefore better support clinical decision-making. We recommend using L-table as a supplement to available techniques of sensitivity analysis.</p><p><strong>Supplementary information: </strong>The online version contains supplementary material available at 10.1007/s10742-022-00282-y.</p>","PeriodicalId":73215,"journal":{"name":"","volume":"23 1","pages":"59-79"},"PeriodicalIF":0.0,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9210342/pdf/","citationCount":"0","resultStr":"{\"title\":\"Addressing unmeasured confounding bias with a prior knowledge guided approach: coronary artery bypass grafting (CABG) versus percutaneous coronary intervention (PCI) in patients with stable ischemic heart disease.\",\"authors\":\"Lewei Duan, Ming-Sum Lee, Jason N Doctor, John L Adams\",\"doi\":\"10.1007/s10742-022-00282-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Unmeasured confounding undermines the validity of observational studies. Although randomized clinical trials (RCTs) are considered the \\\"gold standard\\\" of study types, we often observe divergent findings between RCTs and empirical settings. We present the \\\"L-table\\\", a simulation-based, prior knowledge (e.g., RCTs) guided approach that estimates the true effect adjusting for the potential influence of unmeasured confounders when using observational data. Using electronic health record data from Kaiser Permanente Southern California, we compare the effectiveness of coronary artery bypass grafting (CABG) and percutaneous coronary intervention (PCI) on endpoints at 1, 3, 5, and 10 years for patients with stable ischemic heart disease. We applied the L-table approach to the propensity score adjusted cohort to derive the omitted-confounder-adjusted estimated effects. After the L-table adjustment, CABG patients are 57.6% less likely to encounter major adverse cardiac and cerebrovascular event (MACCE) at 1 year (OR [95% CI] 0.424 [0.396, 0.517]), 56.4% less likely at 3 years (OR [95% CI] 0.436 [0.369, 0.527]), and 48.9% less likely at 5 years (OR [95% CI] 0.511 [0.451, 0.538]). CABG patients are also 49.5% less likely to die by the end of 10 years than PCI patients (OR [95% CI] 0.505 [0.446, 0.582]). We found the estimated true effects all shifted towards CABG as a more effective procedure that led to better health outcomes compared to PCI. Unlike existing sensitivity tools, the L-table approach explicitly lays out probable values and can therefore better support clinical decision-making. We recommend using L-table as a supplement to available techniques of sensitivity analysis.</p><p><strong>Supplementary information: </strong>The online version contains supplementary material available at 10.1007/s10742-022-00282-y.</p>\",\"PeriodicalId\":73215,\"journal\":{\"name\":\"\",\"volume\":\"23 1\",\"pages\":\"59-79\"},\"PeriodicalIF\":0.0,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9210342/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s10742-022-00282-y\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s10742-022-00282-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Addressing unmeasured confounding bias with a prior knowledge guided approach: coronary artery bypass grafting (CABG) versus percutaneous coronary intervention (PCI) in patients with stable ischemic heart disease.
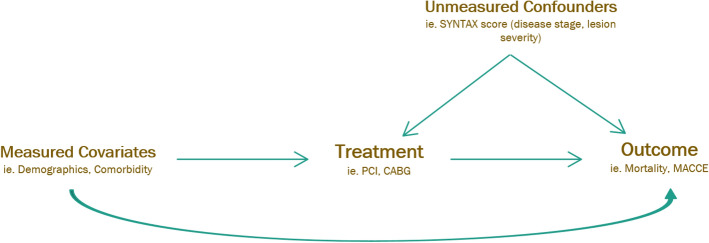
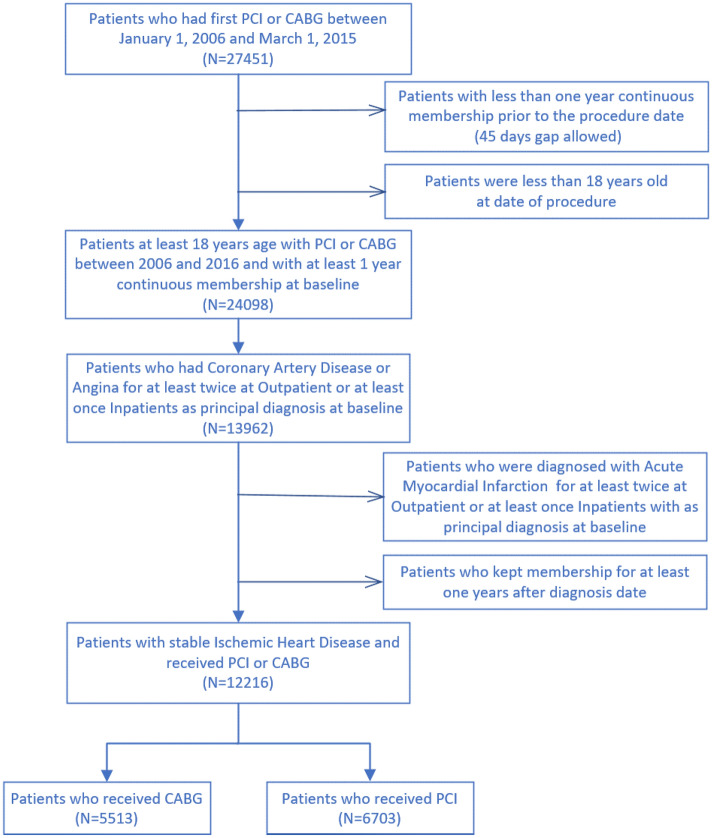
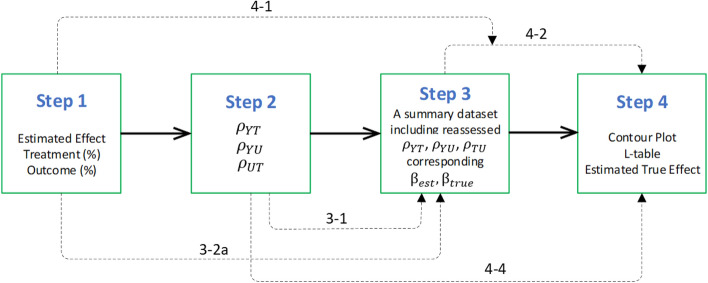
Unmeasured confounding undermines the validity of observational studies. Although randomized clinical trials (RCTs) are considered the "gold standard" of study types, we often observe divergent findings between RCTs and empirical settings. We present the "L-table", a simulation-based, prior knowledge (e.g., RCTs) guided approach that estimates the true effect adjusting for the potential influence of unmeasured confounders when using observational data. Using electronic health record data from Kaiser Permanente Southern California, we compare the effectiveness of coronary artery bypass grafting (CABG) and percutaneous coronary intervention (PCI) on endpoints at 1, 3, 5, and 10 years for patients with stable ischemic heart disease. We applied the L-table approach to the propensity score adjusted cohort to derive the omitted-confounder-adjusted estimated effects. After the L-table adjustment, CABG patients are 57.6% less likely to encounter major adverse cardiac and cerebrovascular event (MACCE) at 1 year (OR [95% CI] 0.424 [0.396, 0.517]), 56.4% less likely at 3 years (OR [95% CI] 0.436 [0.369, 0.527]), and 48.9% less likely at 5 years (OR [95% CI] 0.511 [0.451, 0.538]). CABG patients are also 49.5% less likely to die by the end of 10 years than PCI patients (OR [95% CI] 0.505 [0.446, 0.582]). We found the estimated true effects all shifted towards CABG as a more effective procedure that led to better health outcomes compared to PCI. Unlike existing sensitivity tools, the L-table approach explicitly lays out probable values and can therefore better support clinical decision-making. We recommend using L-table as a supplement to available techniques of sensitivity analysis.
Supplementary information: The online version contains supplementary material available at 10.1007/s10742-022-00282-y.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
