Aisha Alkubaisi, Charles C J Dong, Christopher R Honey
{"title":"迷走神经根内副交感神经纤维的位置:1例报告及文献复习。","authors":"Aisha Alkubaisi, Charles C J Dong, Christopher R Honey","doi":"10.1159/000528094","DOIUrl":null,"url":null,"abstract":"<p><p>The vagus nerve has motor, sensory, and parasympathetic components. Understanding the nerve's internal anatomy, its variations, and relationship to the glossopharyngeal nerve are crucial for neurosurgeons decompressing the lower cranial nerves. We present a case report demonstrating the location of the parasympathetic fibres within the vagus nerve rootlets. A 47-year-old woman presented with a 1-year history of medically refractory left-sided glossopharyngeal neuralgia and a more recent history of left-sided hemi-laryngopharyngeal spasm. magnetic resonance imaging showed her left posterior inferior cerebellar artery distorting the lower cranial nerves on the affected left side. The patient consented to microvascular decompression of the lower cranial nerves with possible sectioning of the glossopharyngeal and upper sensory rootlets of the vagus nerve. During surgery, electrical stimulation of the most caudal rootlet of the vagus nerve triggered profound bradycardia. None of the more rostral rootlets had a similar parasympathetic response. This case is the first demonstration, to our knowledge, of the location of the cardiac parasympathetic fibres within the human vagus nerve rootlets. This new understanding of the vagus nerve rootlets' distribution of pure sensory (most rostral), motor/sensory (more caudal), and parasympathetic (most caudal) fibres may lead to a better understanding and diagnosis of the vagal rhizopathies. Approximately 20% of patients with glossopharyngeal neuralgia also have paroxysmal cough. This could be due to the anatomical juxtaposition of the IXth cranial nerve with the rostral vagal rootlets with pure sensory fibres (which mediate a tickling sensation in the lungs). A subgroup of patients with glossopharyngeal neuralgia have neuralgia-induced syncope. The cause of this rare condition, \"vago-glossopharyngeal neuralgia,\" has been debated since it was first described by Riley in 1942. Our case supports the theory that this neuralgia-induced bradycardia is reflexively mediated through the brainstem with afferent impulses in the IXth and efferent impulses in the Xth cranial nerve. The rarer co-occurrence of glossopharyngeal neuralgia with hemi-laryngopharyngeal spasm (as seen in this case) may be explained by the proximity of the IXth nerve with the more caudal vagus rootlets which have motor (and probably sensory) supply to the throat. Finally, if there is a vagal rhizopathy related to compression of its parasympathetic fibres, one would expect it to be at the most caudal rootlet of the vagus nerve.</p>","PeriodicalId":22078,"journal":{"name":"Stereotactic and Functional Neurosurgery","volume":"101 1","pages":"68-71"},"PeriodicalIF":2.4000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9986834/pdf/","citationCount":"1","resultStr":"{\"title\":\"The Location of the Parasympathetic Fibres within the Vagus Nerve Rootlets: A Case Report and a Review of the Literature.\",\"authors\":\"Aisha Alkubaisi, Charles C J Dong, Christopher R Honey\",\"doi\":\"10.1159/000528094\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The vagus nerve has motor, sensory, and parasympathetic components. Understanding the nerve's internal anatomy, its variations, and relationship to the glossopharyngeal nerve are crucial for neurosurgeons decompressing the lower cranial nerves. We present a case report demonstrating the location of the parasympathetic fibres within the vagus nerve rootlets. A 47-year-old woman presented with a 1-year history of medically refractory left-sided glossopharyngeal neuralgia and a more recent history of left-sided hemi-laryngopharyngeal spasm. magnetic resonance imaging showed her left posterior inferior cerebellar artery distorting the lower cranial nerves on the affected left side. The patient consented to microvascular decompression of the lower cranial nerves with possible sectioning of the glossopharyngeal and upper sensory rootlets of the vagus nerve. During surgery, electrical stimulation of the most caudal rootlet of the vagus nerve triggered profound bradycardia. None of the more rostral rootlets had a similar parasympathetic response. This case is the first demonstration, to our knowledge, of the location of the cardiac parasympathetic fibres within the human vagus nerve rootlets. This new understanding of the vagus nerve rootlets' distribution of pure sensory (most rostral), motor/sensory (more caudal), and parasympathetic (most caudal) fibres may lead to a better understanding and diagnosis of the vagal rhizopathies. Approximately 20% of patients with glossopharyngeal neuralgia also have paroxysmal cough. This could be due to the anatomical juxtaposition of the IXth cranial nerve with the rostral vagal rootlets with pure sensory fibres (which mediate a tickling sensation in the lungs). A subgroup of patients with glossopharyngeal neuralgia have neuralgia-induced syncope. The cause of this rare condition, \\\"vago-glossopharyngeal neuralgia,\\\" has been debated since it was first described by Riley in 1942. Our case supports the theory that this neuralgia-induced bradycardia is reflexively mediated through the brainstem with afferent impulses in the IXth and efferent impulses in the Xth cranial nerve. The rarer co-occurrence of glossopharyngeal neuralgia with hemi-laryngopharyngeal spasm (as seen in this case) may be explained by the proximity of the IXth nerve with the more caudal vagus rootlets which have motor (and probably sensory) supply to the throat. Finally, if there is a vagal rhizopathy related to compression of its parasympathetic fibres, one would expect it to be at the most caudal rootlet of the vagus nerve.</p>\",\"PeriodicalId\":22078,\"journal\":{\"name\":\"Stereotactic and Functional Neurosurgery\",\"volume\":\"101 1\",\"pages\":\"68-71\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9986834/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Stereotactic and Functional Neurosurgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1159/000528094\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"NEUROIMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stereotactic and Functional Neurosurgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000528094","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"NEUROIMAGING","Score":null,"Total":0}
The Location of the Parasympathetic Fibres within the Vagus Nerve Rootlets: A Case Report and a Review of the Literature.
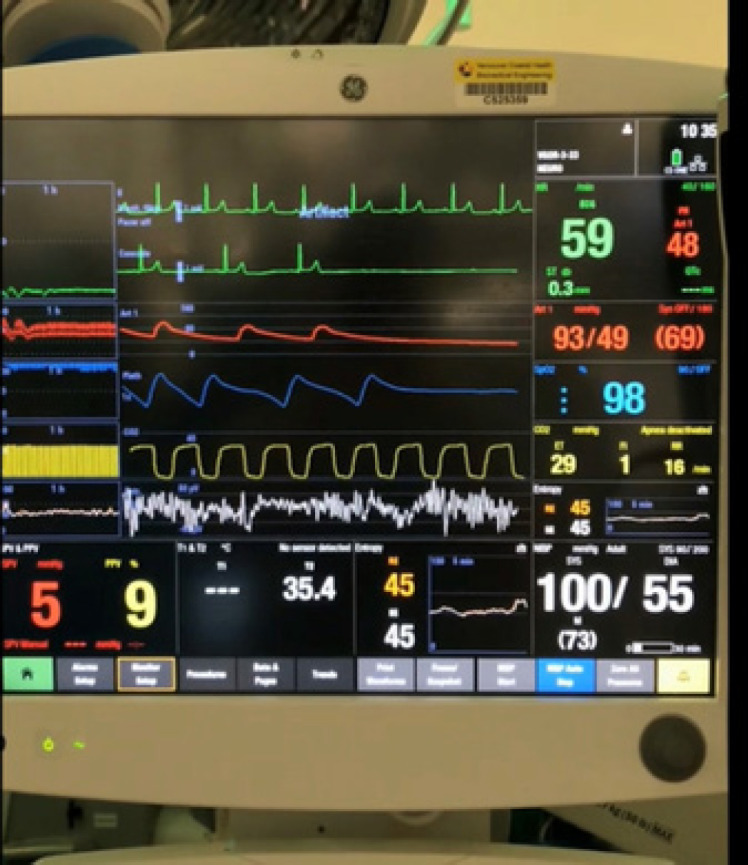
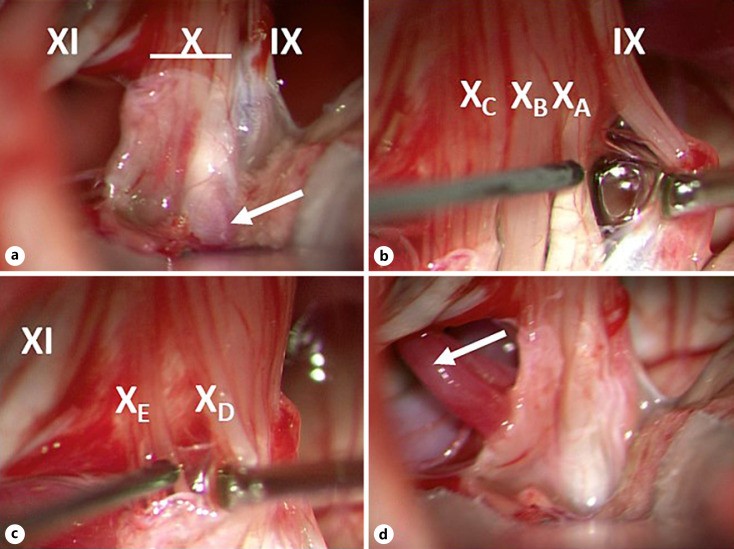
The vagus nerve has motor, sensory, and parasympathetic components. Understanding the nerve's internal anatomy, its variations, and relationship to the glossopharyngeal nerve are crucial for neurosurgeons decompressing the lower cranial nerves. We present a case report demonstrating the location of the parasympathetic fibres within the vagus nerve rootlets. A 47-year-old woman presented with a 1-year history of medically refractory left-sided glossopharyngeal neuralgia and a more recent history of left-sided hemi-laryngopharyngeal spasm. magnetic resonance imaging showed her left posterior inferior cerebellar artery distorting the lower cranial nerves on the affected left side. The patient consented to microvascular decompression of the lower cranial nerves with possible sectioning of the glossopharyngeal and upper sensory rootlets of the vagus nerve. During surgery, electrical stimulation of the most caudal rootlet of the vagus nerve triggered profound bradycardia. None of the more rostral rootlets had a similar parasympathetic response. This case is the first demonstration, to our knowledge, of the location of the cardiac parasympathetic fibres within the human vagus nerve rootlets. This new understanding of the vagus nerve rootlets' distribution of pure sensory (most rostral), motor/sensory (more caudal), and parasympathetic (most caudal) fibres may lead to a better understanding and diagnosis of the vagal rhizopathies. Approximately 20% of patients with glossopharyngeal neuralgia also have paroxysmal cough. This could be due to the anatomical juxtaposition of the IXth cranial nerve with the rostral vagal rootlets with pure sensory fibres (which mediate a tickling sensation in the lungs). A subgroup of patients with glossopharyngeal neuralgia have neuralgia-induced syncope. The cause of this rare condition, "vago-glossopharyngeal neuralgia," has been debated since it was first described by Riley in 1942. Our case supports the theory that this neuralgia-induced bradycardia is reflexively mediated through the brainstem with afferent impulses in the IXth and efferent impulses in the Xth cranial nerve. The rarer co-occurrence of glossopharyngeal neuralgia with hemi-laryngopharyngeal spasm (as seen in this case) may be explained by the proximity of the IXth nerve with the more caudal vagus rootlets which have motor (and probably sensory) supply to the throat. Finally, if there is a vagal rhizopathy related to compression of its parasympathetic fibres, one would expect it to be at the most caudal rootlet of the vagus nerve.
期刊介绍:
''Stereotactic and Functional Neurosurgery'' provides a single source for the reader to keep abreast of developments in the most rapidly advancing subspecialty within neurosurgery. Technological advances in computer-assisted surgery, robotics, imaging and neurophysiology are being applied to clinical problems with ever-increasing rapidity in stereotaxis more than any other field, providing opportunities for new approaches to surgical and radiotherapeutic management of diseases of the brain, spinal cord, and spine. Issues feature advances in the use of deep-brain stimulation, imaging-guided techniques in stereotactic biopsy and craniotomy, stereotactic radiosurgery, and stereotactically implanted and guided radiotherapeutics and biologicals in the treatment of functional and movement disorders, brain tumors, and other diseases of the brain. Background information from basic science laboratories related to such clinical advances provides the reader with an overall perspective of this field. Proceedings and abstracts from many of the key international meetings furnish an overview of this specialty available nowhere else. ''Stereotactic and Functional Neurosurgery'' meets the information needs of both investigators and clinicians in this rapidly advancing field.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
