Alyssa W Tuan, Nauroz Syed, Ronaldo P Panganiban, Roland Y Lee, Shannon Dalessio, Sandeep Pradhan, Junjia Zhu, Ann Ouyang
{"title":"比较芝加哥分类3.0版和4.0版标准诊断为食管运动不良的患者。","authors":"Alyssa W Tuan, Nauroz Syed, Ronaldo P Panganiban, Roland Y Lee, Shannon Dalessio, Sandeep Pradhan, Junjia Zhu, Ann Ouyang","doi":"10.14740/gr1563","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Chicago Classification version 4.0 (CCv4.0) of ineffective esophageal motility (IEM) is more stringent than the Chicago Classification version 3.0 (CCv3.0) definition. We aimed to compare the clinical and manometric features of patients meeting CCv4.0 IEM criteria (group 1) versus patients meeting CCv3.0 IEM but not CCv4.0 criteria (group 2).</p><p><strong>Methods: </strong>We collected retrospective clinical, manometric, endoscopic, and radiographic data on 174 adults diagnosed with IEM from 2011 to 2019. Complete bolus clearance was defined as evidence of exit of the bolus by impedance measurement at all distal recording sites. Barium studies included barium swallow, modified barium swallow, and barium upper gastrointestinal series studies, and collected data from these reports include abnormal motility and delay in the passage of liquid barium or barium tablet. These data along with other clinical and manometric data were analyzed using comparison and correlation tests. All records were reviewed for repeated studies and the stability of the manometric diagnoses.</p><p><strong>Results: </strong>Most demographic and clinical variables were not different between the groups. A lower mean lower esophageal sphincter pressure was correlated with greater percent of ineffective swallows in group 1 (n = 128) (r = -0.2495, P = 0.0050) and not in group 2. In group 1, increased percent of failed contractions on manometry was associated with increased incomplete bolus clearance (r = 0.3689, P = 0.0001). No such association was observed in group 2. A lower median integrated relaxation pressure was correlated with greater percent of ineffective contractions in group 1 (r = -0.1825, P = 0.0407) and not group 2. Symptom of dysphagia was more prevalent (51.6% versus 69.6%, P = 0.0347) in group 2. Dysphagia was not associated with intrabolus pressure, bolus clearance, barium delay, or weak or failed contractions in either group. In the small number of subjects with repeated studies, a CCv4.0 diagnosis appeared more stable over time.</p><p><strong>Conclusions: </strong>CCv4.0 IEM was associated with worse esophageal function indicated by reduced bolus clearance. Most other features studied did not differ. Symptom presentation cannot predict if patients are likely to have IEM by CCv4.0. Dysphagia was not associated with worse motility, suggesting it may not be primarily dependent on bolus transit.</p>","PeriodicalId":12461,"journal":{"name":"Gastroenterology Research","volume":"16 1","pages":"37-49"},"PeriodicalIF":1.7000,"publicationDate":"2023-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f4/cb/gr-16-037.PMC9990528.pdf","citationCount":"3","resultStr":"{\"title\":\"Comparing Patients Diagnosed With Ineffective Esophageal Motility by the Chicago Classification Version 3.0 and Version 4.0 Criteria.\",\"authors\":\"Alyssa W Tuan, Nauroz Syed, Ronaldo P Panganiban, Roland Y Lee, Shannon Dalessio, Sandeep Pradhan, Junjia Zhu, Ann Ouyang\",\"doi\":\"10.14740/gr1563\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The Chicago Classification version 4.0 (CCv4.0) of ineffective esophageal motility (IEM) is more stringent than the Chicago Classification version 3.0 (CCv3.0) definition. We aimed to compare the clinical and manometric features of patients meeting CCv4.0 IEM criteria (group 1) versus patients meeting CCv3.0 IEM but not CCv4.0 criteria (group 2).</p><p><strong>Methods: </strong>We collected retrospective clinical, manometric, endoscopic, and radiographic data on 174 adults diagnosed with IEM from 2011 to 2019. Complete bolus clearance was defined as evidence of exit of the bolus by impedance measurement at all distal recording sites. Barium studies included barium swallow, modified barium swallow, and barium upper gastrointestinal series studies, and collected data from these reports include abnormal motility and delay in the passage of liquid barium or barium tablet. These data along with other clinical and manometric data were analyzed using comparison and correlation tests. All records were reviewed for repeated studies and the stability of the manometric diagnoses.</p><p><strong>Results: </strong>Most demographic and clinical variables were not different between the groups. A lower mean lower esophageal sphincter pressure was correlated with greater percent of ineffective swallows in group 1 (n = 128) (r = -0.2495, P = 0.0050) and not in group 2. In group 1, increased percent of failed contractions on manometry was associated with increased incomplete bolus clearance (r = 0.3689, P = 0.0001). No such association was observed in group 2. A lower median integrated relaxation pressure was correlated with greater percent of ineffective contractions in group 1 (r = -0.1825, P = 0.0407) and not group 2. Symptom of dysphagia was more prevalent (51.6% versus 69.6%, P = 0.0347) in group 2. Dysphagia was not associated with intrabolus pressure, bolus clearance, barium delay, or weak or failed contractions in either group. In the small number of subjects with repeated studies, a CCv4.0 diagnosis appeared more stable over time.</p><p><strong>Conclusions: </strong>CCv4.0 IEM was associated with worse esophageal function indicated by reduced bolus clearance. Most other features studied did not differ. Symptom presentation cannot predict if patients are likely to have IEM by CCv4.0. Dysphagia was not associated with worse motility, suggesting it may not be primarily dependent on bolus transit.</p>\",\"PeriodicalId\":12461,\"journal\":{\"name\":\"Gastroenterology Research\",\"volume\":\"16 1\",\"pages\":\"37-49\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2023-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f4/cb/gr-16-037.PMC9990528.pdf\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gastroenterology Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/gr1563\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastroenterology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/gr1563","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 3
摘要
背景:芝加哥分类4.0版(CCv4.0)对无效食管动力(IEM)的定义比芝加哥分类3.0版(CCv3.0)更为严格。我们的目的是比较符合CCv4.0 IEM标准的患者(1组)与符合CCv3.0 IEM但不符合CCv4.0标准的患者(2组)的临床和血压特征。方法:我们收集了2011年至2019年诊断为IEM的174名成人的回顾性临床、血压、内窥镜和放射学数据。通过在所有远端记录部位的阻抗测量,将完全的弹丸间隙定义为弹丸出口的证据。钡研究包括吞钡、改良吞钡和上胃肠道系列研究,从这些报告中收集的数据包括运动异常和液体钡或钡片的通过延迟。这些数据与其他临床和血压测量数据一起使用比较和相关测试进行分析。对所有记录进行回顾,以确保重复研究和测压诊断的稳定性。结果:大多数人口统计学和临床变量在两组间无差异。组1中食管括约肌平均压力越低,吞咽无效率越高(n = 128) (r = -0.2495, P = 0.0050),组2中则无此关系。在第1组中,测压失败收缩的百分比增加与不完全丸清除增加相关(r = 0.3689, P = 0.0001)。在第二组中没有观察到这种关联。组1较低的中位综合松弛压力与较高的无效收缩率相关(r = -0.1825, P = 0.0407),组2则无相关。第2组患者以吞咽困难为主(51.6%比69.6%,P = 0.0347)。两组的吞咽困难均与肠内压力、肠内清除率、钡延迟或收缩微弱或失败无关。在少数重复研究的受试者中,CCv4.0的诊断随着时间的推移似乎更稳定。结论:CCv4.0 IEM与食道功能恶化相关,表现为丸内清除率降低。研究的大多数其他特征没有差异。症状表现不能预测患者是否可能在CCv4.0时发生IEM。吞咽困难与运动不良无关,提示吞咽困难可能主要不依赖于大剂量转运。
Comparing Patients Diagnosed With Ineffective Esophageal Motility by the Chicago Classification Version 3.0 and Version 4.0 Criteria.
Background: The Chicago Classification version 4.0 (CCv4.0) of ineffective esophageal motility (IEM) is more stringent than the Chicago Classification version 3.0 (CCv3.0) definition. We aimed to compare the clinical and manometric features of patients meeting CCv4.0 IEM criteria (group 1) versus patients meeting CCv3.0 IEM but not CCv4.0 criteria (group 2).
Methods: We collected retrospective clinical, manometric, endoscopic, and radiographic data on 174 adults diagnosed with IEM from 2011 to 2019. Complete bolus clearance was defined as evidence of exit of the bolus by impedance measurement at all distal recording sites. Barium studies included barium swallow, modified barium swallow, and barium upper gastrointestinal series studies, and collected data from these reports include abnormal motility and delay in the passage of liquid barium or barium tablet. These data along with other clinical and manometric data were analyzed using comparison and correlation tests. All records were reviewed for repeated studies and the stability of the manometric diagnoses.
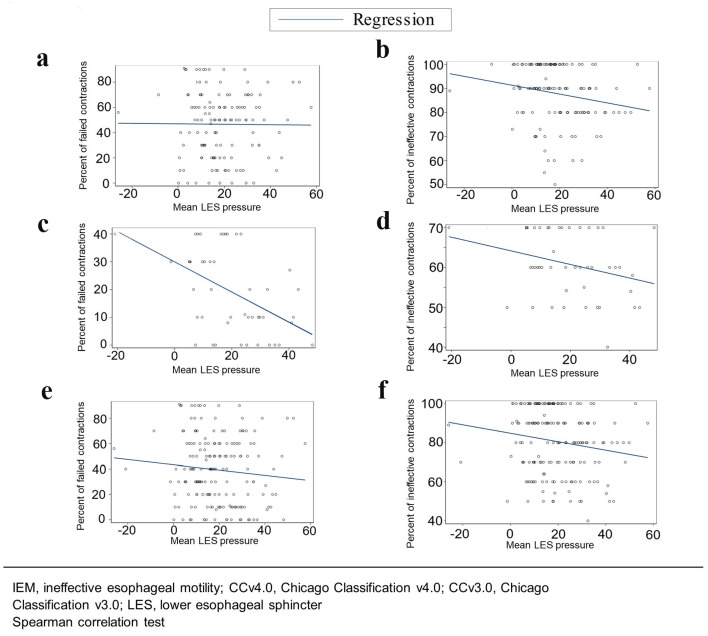
Results: Most demographic and clinical variables were not different between the groups. A lower mean lower esophageal sphincter pressure was correlated with greater percent of ineffective swallows in group 1 (n = 128) (r = -0.2495, P = 0.0050) and not in group 2. In group 1, increased percent of failed contractions on manometry was associated with increased incomplete bolus clearance (r = 0.3689, P = 0.0001). No such association was observed in group 2. A lower median integrated relaxation pressure was correlated with greater percent of ineffective contractions in group 1 (r = -0.1825, P = 0.0407) and not group 2. Symptom of dysphagia was more prevalent (51.6% versus 69.6%, P = 0.0347) in group 2. Dysphagia was not associated with intrabolus pressure, bolus clearance, barium delay, or weak or failed contractions in either group. In the small number of subjects with repeated studies, a CCv4.0 diagnosis appeared more stable over time.
Conclusions: CCv4.0 IEM was associated with worse esophageal function indicated by reduced bolus clearance. Most other features studied did not differ. Symptom presentation cannot predict if patients are likely to have IEM by CCv4.0. Dysphagia was not associated with worse motility, suggesting it may not be primarily dependent on bolus transit.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
