Arvind Nayak, Omar El-Taji, Sugeeta Sukumar, John Piedad, Aruni Ghose, Rob Hughes, Roberto Alonzi, Peter Ostler, Anand Sharma, Tim Lane, Jim Adshead, Nikhil Vasdev
{"title":"单三级癌症中心在机器人辅助腹腔镜前列腺切除术后pT3b前列腺癌的处理经验。","authors":"Arvind Nayak, Omar El-Taji, Sugeeta Sukumar, John Piedad, Aruni Ghose, Rob Hughes, Roberto Alonzi, Peter Ostler, Anand Sharma, Tim Lane, Jim Adshead, Nikhil Vasdev","doi":"10.1097/CU9.0000000000000115","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pathological involvement of the seminal vesicle poses a treatment dilemma following robotic prostatectomy. Margin status plays an important role in deciding further management. A wide range of treatment options are available, including active monitoring, adjuvant radiotherapy, salvage radiotherapy, and occasionally androgen deprivation therapy. Patients undergoing postoperative radiotherapy tend to have higher risk of urinary and bowel morbidities. The recent RADICALS-RT concluded that adjuvant radiotherapy did not have any benefit compared with salvage radiotherapy. We aim to audit the incidence, margin status, and management of T3b cancer cases at our center.</p><p><strong>Materials and methods: </strong>A retrospective analysis was conducted of all patients diagnosed with pathological T3b (pT3b) prostate cancer following robotic-assisted laparoscopic prostatectomy from January 2012 to July 2020. Preoperative parameters analyzed included prostate-specific antigen (PSA), T stage, and age. A chi-square test and 2-tailed <i>t</i> test were used to determine the relationship between categorical and continuous variables, respectively. Kaplan-Meier survival curves were generated to assess overall survival in patients with pT3b prostate cancer and used to compare unadjusted progression-free survival among those who underwent adjuvant and salvage radiotherapy.</p><p><strong>Results: </strong>A total of 83 (5%) of 1665 patients who underwent robotic prostatectomy were diagnosed with pT3b prostate cancer between January 2012 and July 2020. Among these, 36 patients (44%) did not receive any radiotherapy during follow-up, compared with 26 patients (31%) who received adjuvant radiotherapy and 21 (25%) who received salvage radiotherapy. The median age of our cohort was 64 (SD, 6.4) years. Mean PSA at presentation was 12.7 μg/L. Positive margins were seen in 36 patients (43%); however, there was no statistically significant difference between treatment groups (<i>p</i> = 0.49). The median overall survival was 96%. There was no significant difference between the adjuvant and salvage groups in terms of biochemical progression-free survival (<i>p</i> = 0.66). Five-year biochemical progression-free survival was 94% for those in the adjuvant radiotherapy group and 97% for those in the salvage radiotherapy group.</p><p><strong>Conclusions: </strong>Our audit corroborates with the recently concluded RADICALS-RT study, although we had fewer patients with positive margins. Radiotherapy can be avoided in patients with T3b prostate cancer, even if margin is positive, until there is definitive evidence of PSA recurrence. In keeping with the conclusion of RADICALS-RT, salvage radiotherapy may be preferable to adjuvant radiotherapy.</p>","PeriodicalId":39147,"journal":{"name":"Current Urology","volume":"16 4","pages":"227-231"},"PeriodicalIF":1.3000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/16/94/curr-urol-16-227.PMC9875210.pdf","citationCount":"0","resultStr":"{\"title\":\"Single tertiary cancer center experience on the management of pT3b prostate cancer after robotic-assisted laparoscopic prostatectomy.\",\"authors\":\"Arvind Nayak, Omar El-Taji, Sugeeta Sukumar, John Piedad, Aruni Ghose, Rob Hughes, Roberto Alonzi, Peter Ostler, Anand Sharma, Tim Lane, Jim Adshead, Nikhil Vasdev\",\"doi\":\"10.1097/CU9.0000000000000115\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Pathological involvement of the seminal vesicle poses a treatment dilemma following robotic prostatectomy. Margin status plays an important role in deciding further management. A wide range of treatment options are available, including active monitoring, adjuvant radiotherapy, salvage radiotherapy, and occasionally androgen deprivation therapy. Patients undergoing postoperative radiotherapy tend to have higher risk of urinary and bowel morbidities. The recent RADICALS-RT concluded that adjuvant radiotherapy did not have any benefit compared with salvage radiotherapy. We aim to audit the incidence, margin status, and management of T3b cancer cases at our center.</p><p><strong>Materials and methods: </strong>A retrospective analysis was conducted of all patients diagnosed with pathological T3b (pT3b) prostate cancer following robotic-assisted laparoscopic prostatectomy from January 2012 to July 2020. Preoperative parameters analyzed included prostate-specific antigen (PSA), T stage, and age. A chi-square test and 2-tailed <i>t</i> test were used to determine the relationship between categorical and continuous variables, respectively. Kaplan-Meier survival curves were generated to assess overall survival in patients with pT3b prostate cancer and used to compare unadjusted progression-free survival among those who underwent adjuvant and salvage radiotherapy.</p><p><strong>Results: </strong>A total of 83 (5%) of 1665 patients who underwent robotic prostatectomy were diagnosed with pT3b prostate cancer between January 2012 and July 2020. Among these, 36 patients (44%) did not receive any radiotherapy during follow-up, compared with 26 patients (31%) who received adjuvant radiotherapy and 21 (25%) who received salvage radiotherapy. The median age of our cohort was 64 (SD, 6.4) years. Mean PSA at presentation was 12.7 μg/L. Positive margins were seen in 36 patients (43%); however, there was no statistically significant difference between treatment groups (<i>p</i> = 0.49). The median overall survival was 96%. There was no significant difference between the adjuvant and salvage groups in terms of biochemical progression-free survival (<i>p</i> = 0.66). Five-year biochemical progression-free survival was 94% for those in the adjuvant radiotherapy group and 97% for those in the salvage radiotherapy group.</p><p><strong>Conclusions: </strong>Our audit corroborates with the recently concluded RADICALS-RT study, although we had fewer patients with positive margins. Radiotherapy can be avoided in patients with T3b prostate cancer, even if margin is positive, until there is definitive evidence of PSA recurrence. In keeping with the conclusion of RADICALS-RT, salvage radiotherapy may be preferable to adjuvant radiotherapy.</p>\",\"PeriodicalId\":39147,\"journal\":{\"name\":\"Current Urology\",\"volume\":\"16 4\",\"pages\":\"227-231\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/16/94/curr-urol-16-227.PMC9875210.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Current Urology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CU9.0000000000000115\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CU9.0000000000000115","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Single tertiary cancer center experience on the management of pT3b prostate cancer after robotic-assisted laparoscopic prostatectomy.
Background: Pathological involvement of the seminal vesicle poses a treatment dilemma following robotic prostatectomy. Margin status plays an important role in deciding further management. A wide range of treatment options are available, including active monitoring, adjuvant radiotherapy, salvage radiotherapy, and occasionally androgen deprivation therapy. Patients undergoing postoperative radiotherapy tend to have higher risk of urinary and bowel morbidities. The recent RADICALS-RT concluded that adjuvant radiotherapy did not have any benefit compared with salvage radiotherapy. We aim to audit the incidence, margin status, and management of T3b cancer cases at our center.
Materials and methods: A retrospective analysis was conducted of all patients diagnosed with pathological T3b (pT3b) prostate cancer following robotic-assisted laparoscopic prostatectomy from January 2012 to July 2020. Preoperative parameters analyzed included prostate-specific antigen (PSA), T stage, and age. A chi-square test and 2-tailed t test were used to determine the relationship between categorical and continuous variables, respectively. Kaplan-Meier survival curves were generated to assess overall survival in patients with pT3b prostate cancer and used to compare unadjusted progression-free survival among those who underwent adjuvant and salvage radiotherapy.
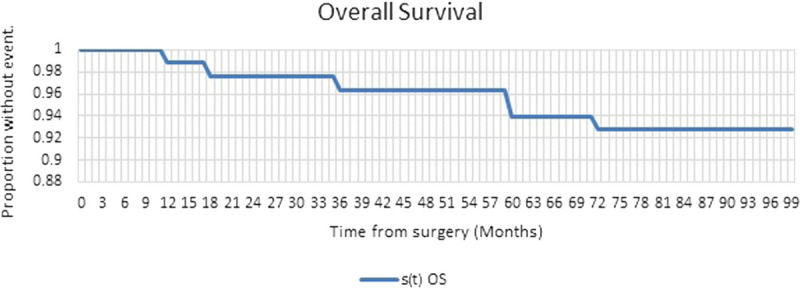
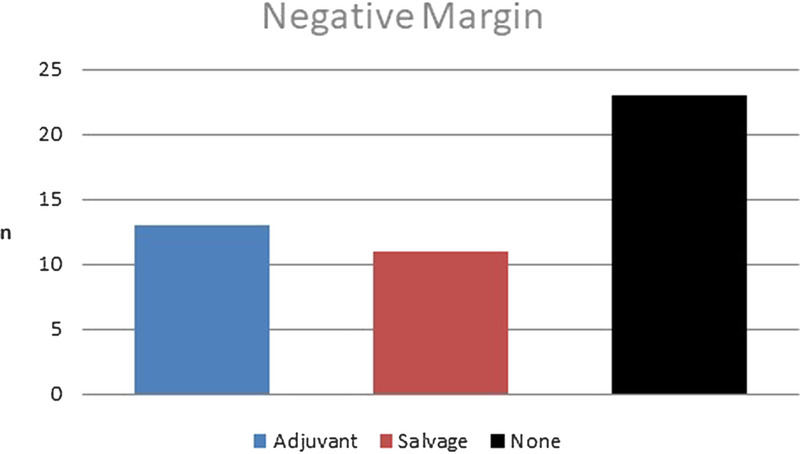
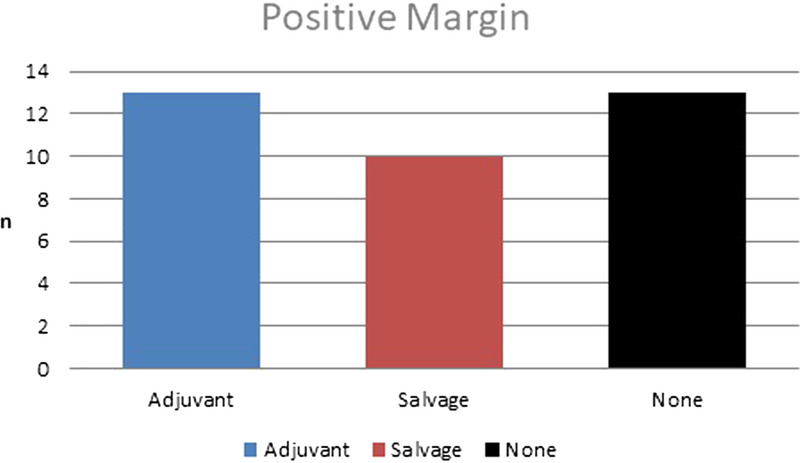
Results: A total of 83 (5%) of 1665 patients who underwent robotic prostatectomy were diagnosed with pT3b prostate cancer between January 2012 and July 2020. Among these, 36 patients (44%) did not receive any radiotherapy during follow-up, compared with 26 patients (31%) who received adjuvant radiotherapy and 21 (25%) who received salvage radiotherapy. The median age of our cohort was 64 (SD, 6.4) years. Mean PSA at presentation was 12.7 μg/L. Positive margins were seen in 36 patients (43%); however, there was no statistically significant difference between treatment groups (p = 0.49). The median overall survival was 96%. There was no significant difference between the adjuvant and salvage groups in terms of biochemical progression-free survival (p = 0.66). Five-year biochemical progression-free survival was 94% for those in the adjuvant radiotherapy group and 97% for those in the salvage radiotherapy group.
Conclusions: Our audit corroborates with the recently concluded RADICALS-RT study, although we had fewer patients with positive margins. Radiotherapy can be avoided in patients with T3b prostate cancer, even if margin is positive, until there is definitive evidence of PSA recurrence. In keeping with the conclusion of RADICALS-RT, salvage radiotherapy may be preferable to adjuvant radiotherapy.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
