Rocco Simone Flammia, Benedikt Hoeh, Francesco Chierigo, Lukas Hohenhorst, Gabriele Sorce, Zhen Tian, Costantino Leonardo, Markus Graefen, Carlo Terrone, Fred Saad, Shahrokh F Shariat, Alberto Briganti, Francesco Montorsi, Felix K H Chun, Michele Gallucci, Pierre I Karakiewicz
{"title":"美国SEER登记的国家综合癌症网络中有利、不利的中高危前列腺癌盆腔淋巴结清扫率的差异","authors":"Rocco Simone Flammia, Benedikt Hoeh, Francesco Chierigo, Lukas Hohenhorst, Gabriele Sorce, Zhen Tian, Costantino Leonardo, Markus Graefen, Carlo Terrone, Fred Saad, Shahrokh F Shariat, Alberto Briganti, Francesco Montorsi, Felix K H Chun, Michele Gallucci, Pierre I Karakiewicz","doi":"10.1097/CU9.0000000000000132","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The National Comprehensive Cancer Network (NCCN) guidelines recommend pelvic lymph node dissection (PLND) in NCCN high- and intermediate-risk prostate cancer patients. We tested for PLND nonadherence (no-PLND) rates within the Surveillance Epidemiology and End Results (2010-2015).</p><p><strong>Materials and methods: </strong>We identified all radical prostatectomy patients who fulfilled the NCCN PLND guideline criteria (n = 23,495). Nonadherence rates to PLND were tabulated and further stratified according to NCCN risk subgroups, race/ethnicity, geographic distribution, and year of diagnosis.</p><p><strong>Results: </strong>Overall, the no-PLND rate was 26%; it was 41%, 25%, and 11% in the NCCN intermediate favorable, intermediate unfavorable, and high-risk prostate cancer patients, respectively (<i>p</i> < 0.001). Over time, the no-PLND rates declined in the overall cohort and within each NCCN risk subgroup. Georgia exhibited the highest no-PLND rate (49%), whereas New Jersey exhibited the lowest (15%). Finally, no-PLND race/ethnicity differences were recorded only in the NCCN intermediate unfavorable subgroup, where Asians exhibited the lowest no-PLND rate (20%) versus African Americans (27%) versus Whites (26%) versus Hispanic-Latinos (25%).</p><p><strong>Conclusions: </strong>The lowest no-PLND rates were recorded in the NCCN high-risk patients followed by NCCN intermediate unfavorable and favorable risk in that order. Our findings suggest that unexpectedly elevated differences in no-PLND rates warrant further examination. In all the NCCN risk subgroups, the no-PLND rates decreased over time.</p>","PeriodicalId":39147,"journal":{"name":"Current Urology","volume":"16 4","pages":"191-196"},"PeriodicalIF":1.3000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a6/c7/curr-urol-16-191.PMC9875209.pdf","citationCount":"1","resultStr":"{\"title\":\"Differences in rates of pelvic lymph node dissection in National Comprehensive Cancer Network favorable, unfavorable intermediate- and high-risk prostate cancer across United States SEER registries.\",\"authors\":\"Rocco Simone Flammia, Benedikt Hoeh, Francesco Chierigo, Lukas Hohenhorst, Gabriele Sorce, Zhen Tian, Costantino Leonardo, Markus Graefen, Carlo Terrone, Fred Saad, Shahrokh F Shariat, Alberto Briganti, Francesco Montorsi, Felix K H Chun, Michele Gallucci, Pierre I Karakiewicz\",\"doi\":\"10.1097/CU9.0000000000000132\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The National Comprehensive Cancer Network (NCCN) guidelines recommend pelvic lymph node dissection (PLND) in NCCN high- and intermediate-risk prostate cancer patients. We tested for PLND nonadherence (no-PLND) rates within the Surveillance Epidemiology and End Results (2010-2015).</p><p><strong>Materials and methods: </strong>We identified all radical prostatectomy patients who fulfilled the NCCN PLND guideline criteria (n = 23,495). Nonadherence rates to PLND were tabulated and further stratified according to NCCN risk subgroups, race/ethnicity, geographic distribution, and year of diagnosis.</p><p><strong>Results: </strong>Overall, the no-PLND rate was 26%; it was 41%, 25%, and 11% in the NCCN intermediate favorable, intermediate unfavorable, and high-risk prostate cancer patients, respectively (<i>p</i> < 0.001). Over time, the no-PLND rates declined in the overall cohort and within each NCCN risk subgroup. Georgia exhibited the highest no-PLND rate (49%), whereas New Jersey exhibited the lowest (15%). Finally, no-PLND race/ethnicity differences were recorded only in the NCCN intermediate unfavorable subgroup, where Asians exhibited the lowest no-PLND rate (20%) versus African Americans (27%) versus Whites (26%) versus Hispanic-Latinos (25%).</p><p><strong>Conclusions: </strong>The lowest no-PLND rates were recorded in the NCCN high-risk patients followed by NCCN intermediate unfavorable and favorable risk in that order. Our findings suggest that unexpectedly elevated differences in no-PLND rates warrant further examination. In all the NCCN risk subgroups, the no-PLND rates decreased over time.</p>\",\"PeriodicalId\":39147,\"journal\":{\"name\":\"Current Urology\",\"volume\":\"16 4\",\"pages\":\"191-196\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a6/c7/curr-urol-16-191.PMC9875209.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Current Urology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CU9.0000000000000132\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CU9.0000000000000132","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Differences in rates of pelvic lymph node dissection in National Comprehensive Cancer Network favorable, unfavorable intermediate- and high-risk prostate cancer across United States SEER registries.
Background: The National Comprehensive Cancer Network (NCCN) guidelines recommend pelvic lymph node dissection (PLND) in NCCN high- and intermediate-risk prostate cancer patients. We tested for PLND nonadherence (no-PLND) rates within the Surveillance Epidemiology and End Results (2010-2015).
Materials and methods: We identified all radical prostatectomy patients who fulfilled the NCCN PLND guideline criteria (n = 23,495). Nonadherence rates to PLND were tabulated and further stratified according to NCCN risk subgroups, race/ethnicity, geographic distribution, and year of diagnosis.
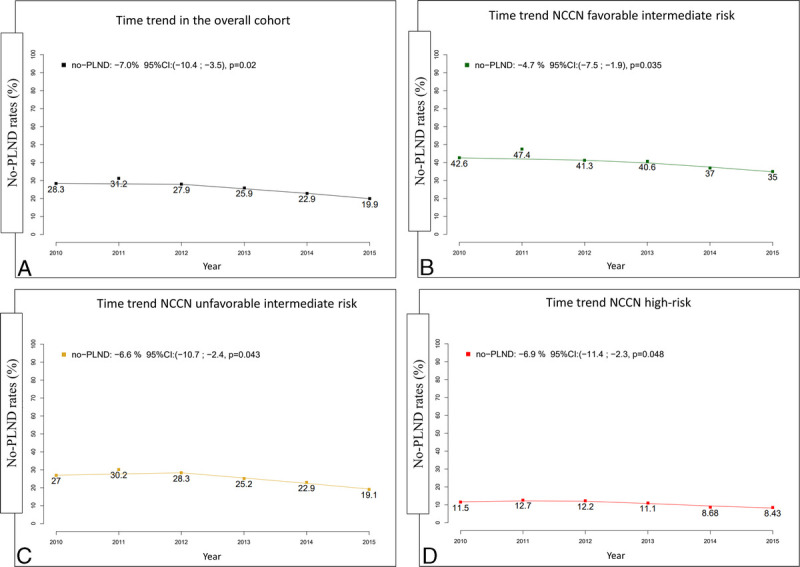
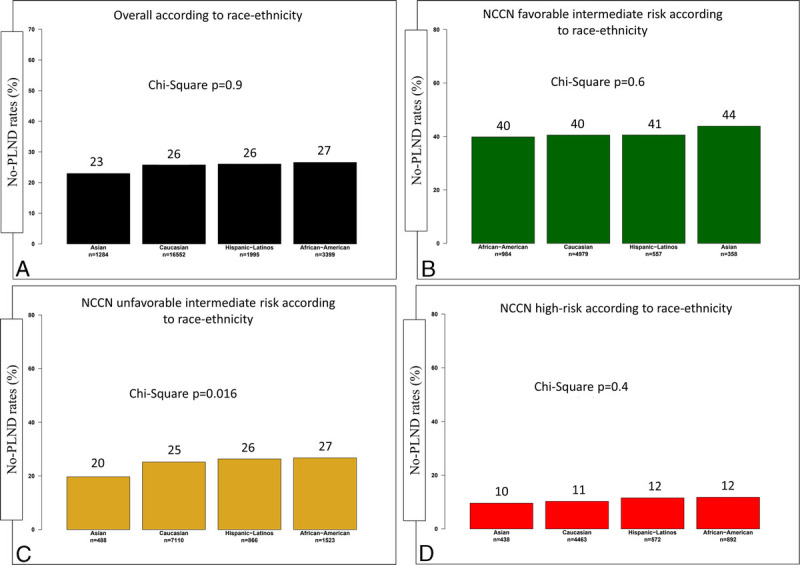
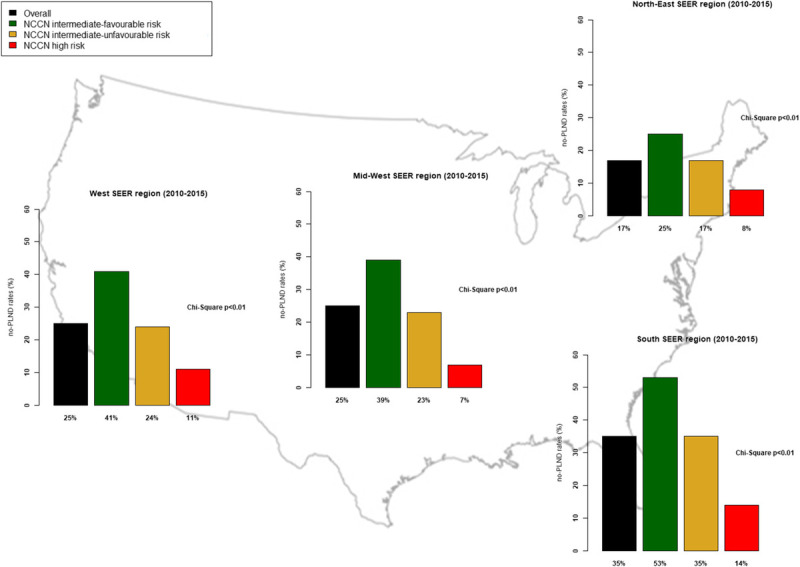
Results: Overall, the no-PLND rate was 26%; it was 41%, 25%, and 11% in the NCCN intermediate favorable, intermediate unfavorable, and high-risk prostate cancer patients, respectively (p < 0.001). Over time, the no-PLND rates declined in the overall cohort and within each NCCN risk subgroup. Georgia exhibited the highest no-PLND rate (49%), whereas New Jersey exhibited the lowest (15%). Finally, no-PLND race/ethnicity differences were recorded only in the NCCN intermediate unfavorable subgroup, where Asians exhibited the lowest no-PLND rate (20%) versus African Americans (27%) versus Whites (26%) versus Hispanic-Latinos (25%).
Conclusions: The lowest no-PLND rates were recorded in the NCCN high-risk patients followed by NCCN intermediate unfavorable and favorable risk in that order. Our findings suggest that unexpectedly elevated differences in no-PLND rates warrant further examination. In all the NCCN risk subgroups, the no-PLND rates decreased over time.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
