Mafalda João, Susana Alves, Miguel Areia, Luís Elvas, Daniel Brito, Sandra Saraiva, Raquel Martins, Ana Teresa Cadime
{"title":"帽辅助内镜粘膜切除术治疗直肠神经内分泌肿瘤:一种有效的选择。","authors":"Mafalda João, Susana Alves, Miguel Areia, Luís Elvas, Daniel Brito, Sandra Saraiva, Raquel Martins, Ana Teresa Cadime","doi":"10.1159/000525964","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The incidence of rectal neuroendocrine tumors (r-NETs) is increasing, and most small r-NETs can be treated endoscopically. The optimal endoscopic approach is still debatable. Conventional endoscopic mucosal resection (EMR) leads to frequent incomplete resection. Endoscopic submucosal dissection (ESD) allows higher complete resection rates but is also associated with higher complication rates. According to some studies, cap-assisted EMR (EMR-C) is an effective and safe alternative for endoscopic resection of r-NETs.</p><p><strong>Aims: </strong>This study aimed to evaluate the efficacy and safety of EMR-C for r-NETs ≤10 mm without muscularis propria invasion or lymphovascular infiltration.</p><p><strong>Methods: </strong>Single-center prospective study including consecutive patients with r-NETs ≤10 mm without muscularis propria invasion or lymphovascular invasion confirmed by endoscopic ultrasound (EUS), submitted to EMR-C between January 2017 and September 2021. Demographic, endoscopic, histopathologic, and follow-up data were retrieved from medical records.</p><p><strong>Results: </strong>A total of 13 patients (male: 54%; <i>n</i> = 7) with a median age of 64 (interquartile range: 54-76) years were included. Most lesions were located at the lower rectum (69.2%, <i>n</i> = 9), and median lesion size was 6 (interquartile range: 4.5-7.5) mm. On EUS evaluation, 69.2% (<i>n</i> = 9) of tumors were limited to muscularis mucosa. EUS accuracy for the depth of invasion was 84.6%. We found a strong correlation between size measurements by histology and EUS (<i>r</i> = 0.83, <i>p</i> < 0.01). Overall, 15.4% (<i>n</i> = 2) were recurrent r-NETs and had been pretreated by conventional EMR. Resection was histologically complete in 92% (n = 12) of cases. Histologic analysis revealed grade 1 tumor in 76.9% (<i>n</i> = 10) of cases. Ki-67 index was inferior to 3% in 84.6% (<i>n</i> = 11) of cases. The median procedure time was 5 (interquartile range: 4-8) min. Only 1 case of intraprocedural bleeding was reported and was successfully controlled endoscopically. Follow-up was available in 92% (<i>n</i> = 12) of cases with a median follow-up of 6 (interquartile range: 12-24) months with no evidence of residual or recurrent lesion on endoscopic or EUS evaluation.</p><p><strong>Conclusion: </strong>EMR-C is fast, safe, and effective for resection of small r-NETs without high-risk features. EUS accurately assesses risk factors. Prospective comparative trials are needed to define the best endoscopic approach.</p>","PeriodicalId":51838,"journal":{"name":"GE Portuguese Journal of Gastroenterology","volume":null,"pages":null},"PeriodicalIF":1.0000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5e/89/pjg-0030-0107.PMC10050888.pdf","citationCount":"1","resultStr":"{\"title\":\"Cap-Assisted Endoscopic Mucosal Resection for Rectal Neuroendocrine Tumors: An Effective Option.\",\"authors\":\"Mafalda João, Susana Alves, Miguel Areia, Luís Elvas, Daniel Brito, Sandra Saraiva, Raquel Martins, Ana Teresa Cadime\",\"doi\":\"10.1159/000525964\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The incidence of rectal neuroendocrine tumors (r-NETs) is increasing, and most small r-NETs can be treated endoscopically. The optimal endoscopic approach is still debatable. Conventional endoscopic mucosal resection (EMR) leads to frequent incomplete resection. Endoscopic submucosal dissection (ESD) allows higher complete resection rates but is also associated with higher complication rates. According to some studies, cap-assisted EMR (EMR-C) is an effective and safe alternative for endoscopic resection of r-NETs.</p><p><strong>Aims: </strong>This study aimed to evaluate the efficacy and safety of EMR-C for r-NETs ≤10 mm without muscularis propria invasion or lymphovascular infiltration.</p><p><strong>Methods: </strong>Single-center prospective study including consecutive patients with r-NETs ≤10 mm without muscularis propria invasion or lymphovascular invasion confirmed by endoscopic ultrasound (EUS), submitted to EMR-C between January 2017 and September 2021. Demographic, endoscopic, histopathologic, and follow-up data were retrieved from medical records.</p><p><strong>Results: </strong>A total of 13 patients (male: 54%; <i>n</i> = 7) with a median age of 64 (interquartile range: 54-76) years were included. Most lesions were located at the lower rectum (69.2%, <i>n</i> = 9), and median lesion size was 6 (interquartile range: 4.5-7.5) mm. On EUS evaluation, 69.2% (<i>n</i> = 9) of tumors were limited to muscularis mucosa. EUS accuracy for the depth of invasion was 84.6%. We found a strong correlation between size measurements by histology and EUS (<i>r</i> = 0.83, <i>p</i> < 0.01). Overall, 15.4% (<i>n</i> = 2) were recurrent r-NETs and had been pretreated by conventional EMR. Resection was histologically complete in 92% (n = 12) of cases. Histologic analysis revealed grade 1 tumor in 76.9% (<i>n</i> = 10) of cases. Ki-67 index was inferior to 3% in 84.6% (<i>n</i> = 11) of cases. The median procedure time was 5 (interquartile range: 4-8) min. Only 1 case of intraprocedural bleeding was reported and was successfully controlled endoscopically. Follow-up was available in 92% (<i>n</i> = 12) of cases with a median follow-up of 6 (interquartile range: 12-24) months with no evidence of residual or recurrent lesion on endoscopic or EUS evaluation.</p><p><strong>Conclusion: </strong>EMR-C is fast, safe, and effective for resection of small r-NETs without high-risk features. EUS accurately assesses risk factors. Prospective comparative trials are needed to define the best endoscopic approach.</p>\",\"PeriodicalId\":51838,\"journal\":{\"name\":\"GE Portuguese Journal of Gastroenterology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2023-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5e/89/pjg-0030-0107.PMC10050888.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"GE Portuguese Journal of Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000525964\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"GE Portuguese Journal of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000525964","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Cap-Assisted Endoscopic Mucosal Resection for Rectal Neuroendocrine Tumors: An Effective Option.
Introduction: The incidence of rectal neuroendocrine tumors (r-NETs) is increasing, and most small r-NETs can be treated endoscopically. The optimal endoscopic approach is still debatable. Conventional endoscopic mucosal resection (EMR) leads to frequent incomplete resection. Endoscopic submucosal dissection (ESD) allows higher complete resection rates but is also associated with higher complication rates. According to some studies, cap-assisted EMR (EMR-C) is an effective and safe alternative for endoscopic resection of r-NETs.
Aims: This study aimed to evaluate the efficacy and safety of EMR-C for r-NETs ≤10 mm without muscularis propria invasion or lymphovascular infiltration.
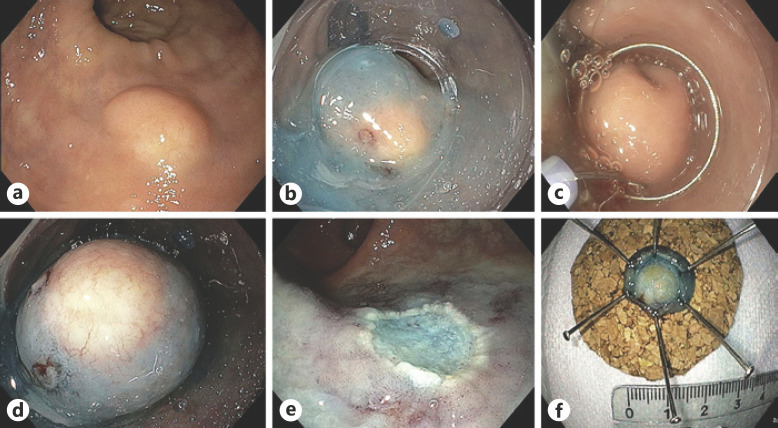
Methods: Single-center prospective study including consecutive patients with r-NETs ≤10 mm without muscularis propria invasion or lymphovascular invasion confirmed by endoscopic ultrasound (EUS), submitted to EMR-C between January 2017 and September 2021. Demographic, endoscopic, histopathologic, and follow-up data were retrieved from medical records.
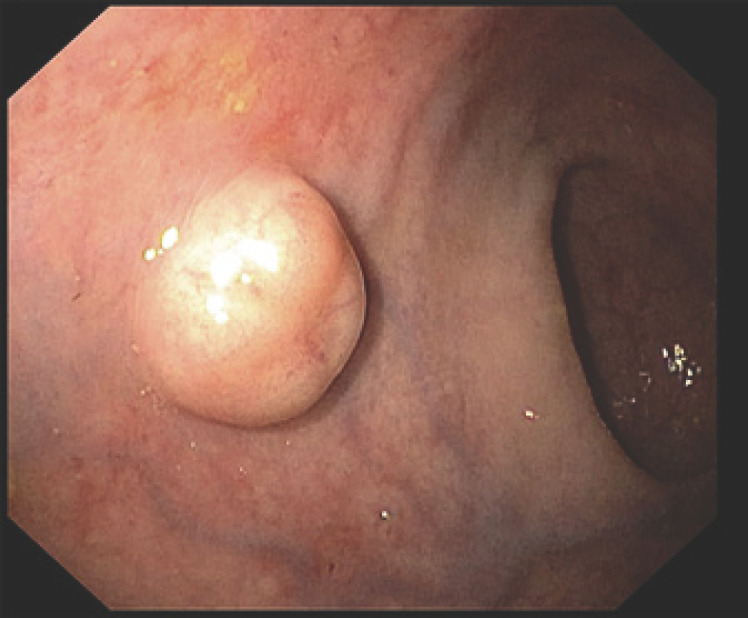
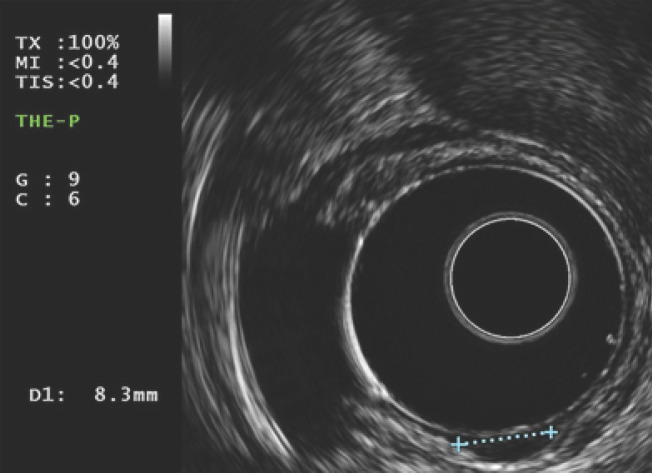
Results: A total of 13 patients (male: 54%; n = 7) with a median age of 64 (interquartile range: 54-76) years were included. Most lesions were located at the lower rectum (69.2%, n = 9), and median lesion size was 6 (interquartile range: 4.5-7.5) mm. On EUS evaluation, 69.2% (n = 9) of tumors were limited to muscularis mucosa. EUS accuracy for the depth of invasion was 84.6%. We found a strong correlation between size measurements by histology and EUS (r = 0.83, p < 0.01). Overall, 15.4% (n = 2) were recurrent r-NETs and had been pretreated by conventional EMR. Resection was histologically complete in 92% (n = 12) of cases. Histologic analysis revealed grade 1 tumor in 76.9% (n = 10) of cases. Ki-67 index was inferior to 3% in 84.6% (n = 11) of cases. The median procedure time was 5 (interquartile range: 4-8) min. Only 1 case of intraprocedural bleeding was reported and was successfully controlled endoscopically. Follow-up was available in 92% (n = 12) of cases with a median follow-up of 6 (interquartile range: 12-24) months with no evidence of residual or recurrent lesion on endoscopic or EUS evaluation.
Conclusion: EMR-C is fast, safe, and effective for resection of small r-NETs without high-risk features. EUS accurately assesses risk factors. Prospective comparative trials are needed to define the best endoscopic approach.
期刊介绍:
The ''GE Portuguese Journal of Gastroenterology'' (formerly Jornal Português de Gastrenterologia), founded in 1994, is the official publication of Sociedade Portuguesa de Gastrenterologia (Portuguese Society of Gastroenterology), Sociedade Portuguesa de Endoscopia Digestiva (Portuguese Society of Digestive Endoscopy) and Associação Portuguesa para o Estudo do Fígado (Portuguese Association for the Study of the Liver). The journal publishes clinical and basic research articles on Gastroenterology, Digestive Endoscopy, Hepatology and related topics. Review articles, clinical case studies, images, letters to the editor and other articles such as recommendations or papers on gastroenterology clinical practice are also considered. Only articles written in English are accepted.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
