{"title":"IgA肾病和非典型抗gbm疾病:儿童快速进展性肾小球肾炎的罕见双重病理。","authors":"Varun Bajaj, Shilpi Thakur, Adarsh Barwad, Aditi Sinha, Arvind Bagga, Geetika Singh","doi":"10.1159/000521582","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Anti-GBM nephritis in the pediatric age group is exceedingly rare with concurrent additional pathologies being even rarer. Tissue diagnosis requires a combination of crescentic histomorphology, immunofluorescence showing \"paint brush stroke\" pattern of linear IgG or rarely IgA, and serum anti-GBM antibodies subject to the disease course and treatment. The authors describe one such case with a dual pathology involving IgA nephropathy and atypical anti-GBM disease.</p><p><strong>Case presentation: </strong>A 13-year-old girl presenting with features of rapidly progressive glomerulonephritis underwent a renal biopsy showing a mesangioproliferative histology with crescents and an immunofluorescence pattern indicating a dual pathology of IgA nephropathy and anti-GBM nephritis. Additional ancillary testing including staining for IgG subclasses and galactose-deficient IgA (KM55) helped to confirm the diagnosis. She responded to steroid pulses and plasma exchange therapy, was off dialysis after 8 weeks with a serum creatinine level of 1.5 mg/dL, and however remains proteinuric at last follow-up.</p><p><strong>Conclusion: </strong>Concurrent anti-GBM nephritis and IgA nephropathy is a rare occurrence and possibly arises from a complex interaction between the anti-GBM antibodies and the basement membrane unmasking the antigens for IgA antibodies. Additional newer techniques like immunofluorescence for KM55 are helpful in establishing the dual pathology.</p>","PeriodicalId":73177,"journal":{"name":"Glomerular diseases","volume":"2 1","pages":"54-57"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ae/06/gdz-0002-0054.PMC9677737.pdf","citationCount":"2","resultStr":"{\"title\":\"IgA Nephropathy and Atypical Anti-GBM Disease: A Rare Dual Pathology in a Pediatric Rapidly Progressive Glomerulonephritis.\",\"authors\":\"Varun Bajaj, Shilpi Thakur, Adarsh Barwad, Aditi Sinha, Arvind Bagga, Geetika Singh\",\"doi\":\"10.1159/000521582\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Anti-GBM nephritis in the pediatric age group is exceedingly rare with concurrent additional pathologies being even rarer. Tissue diagnosis requires a combination of crescentic histomorphology, immunofluorescence showing \\\"paint brush stroke\\\" pattern of linear IgG or rarely IgA, and serum anti-GBM antibodies subject to the disease course and treatment. The authors describe one such case with a dual pathology involving IgA nephropathy and atypical anti-GBM disease.</p><p><strong>Case presentation: </strong>A 13-year-old girl presenting with features of rapidly progressive glomerulonephritis underwent a renal biopsy showing a mesangioproliferative histology with crescents and an immunofluorescence pattern indicating a dual pathology of IgA nephropathy and anti-GBM nephritis. Additional ancillary testing including staining for IgG subclasses and galactose-deficient IgA (KM55) helped to confirm the diagnosis. She responded to steroid pulses and plasma exchange therapy, was off dialysis after 8 weeks with a serum creatinine level of 1.5 mg/dL, and however remains proteinuric at last follow-up.</p><p><strong>Conclusion: </strong>Concurrent anti-GBM nephritis and IgA nephropathy is a rare occurrence and possibly arises from a complex interaction between the anti-GBM antibodies and the basement membrane unmasking the antigens for IgA antibodies. Additional newer techniques like immunofluorescence for KM55 are helpful in establishing the dual pathology.</p>\",\"PeriodicalId\":73177,\"journal\":{\"name\":\"Glomerular diseases\",\"volume\":\"2 1\",\"pages\":\"54-57\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ae/06/gdz-0002-0054.PMC9677737.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Glomerular diseases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000521582\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Glomerular diseases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000521582","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
IgA Nephropathy and Atypical Anti-GBM Disease: A Rare Dual Pathology in a Pediatric Rapidly Progressive Glomerulonephritis.
Introduction: Anti-GBM nephritis in the pediatric age group is exceedingly rare with concurrent additional pathologies being even rarer. Tissue diagnosis requires a combination of crescentic histomorphology, immunofluorescence showing "paint brush stroke" pattern of linear IgG or rarely IgA, and serum anti-GBM antibodies subject to the disease course and treatment. The authors describe one such case with a dual pathology involving IgA nephropathy and atypical anti-GBM disease.
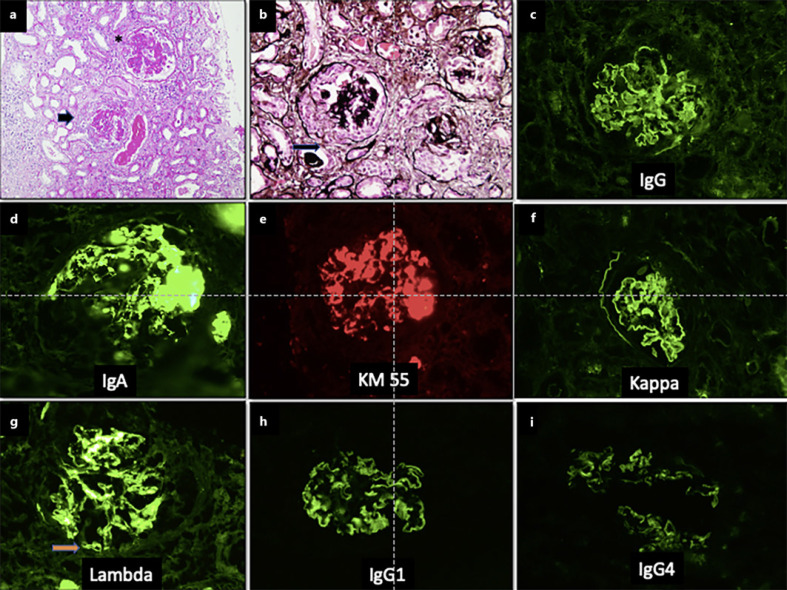
Case presentation: A 13-year-old girl presenting with features of rapidly progressive glomerulonephritis underwent a renal biopsy showing a mesangioproliferative histology with crescents and an immunofluorescence pattern indicating a dual pathology of IgA nephropathy and anti-GBM nephritis. Additional ancillary testing including staining for IgG subclasses and galactose-deficient IgA (KM55) helped to confirm the diagnosis. She responded to steroid pulses and plasma exchange therapy, was off dialysis after 8 weeks with a serum creatinine level of 1.5 mg/dL, and however remains proteinuric at last follow-up.
Conclusion: Concurrent anti-GBM nephritis and IgA nephropathy is a rare occurrence and possibly arises from a complex interaction between the anti-GBM antibodies and the basement membrane unmasking the antigens for IgA antibodies. Additional newer techniques like immunofluorescence for KM55 are helpful in establishing the dual pathology.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
