{"title":"系统性红斑狼疮相关免疫血小板减少症显著复发的风险因素和适当的维持治疗策略。","authors":"He-Jun Li, Yi-Qing Zheng, Ling Chen, Shun-Ping Lin, Xiang-Xiong Zheng","doi":"10.1177/20406223231160688","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Systemic lupus erythematosus-associated immune thrombocytopenia (SLE-ITP) is characterized by relapse. The risk factors of relapse and appropriate maintenance therapy strategy deserve further exploration.</p><p><strong>Objectives: </strong>To determine the risk factors for relapse and appropriate maintenance therapy in significant SLE-ITP patients (a platelet count ⩽30 × 10<sup>9</sup>/l) after the first complete response.</p><p><strong>Design: </strong>Retrospective cohort study using the medical records of 105 patients diagnosed as significant SLE-ITP in Fujian Medical University Union Hospital during December 2012 to March 2021. Patients were followed through a call for observations in January 2022.</p><p><strong>Methods: </strong>Data including demographics, initial clinical feature, induction and maintenance therapy, and outcome at the end of follow-up were analyzed. Risk factors for significant relapse were analyzed using multivariate logistic regression models. The cumulative hazard of significant relapse and the duration of response were estimated, and the differences in outcome between groups were compared using the Cox regression analysis.</p><p><strong>Results: </strong>A total of 65 significant SLE-ITP patients were eligible for the final analysis. Median [interquartile range (IQR)] follow-up duration and median [IQR] duration of response were 62.2 [41.0-79.6] months and 43.4 [20.3-68.7] months, respectively. After the first complete response, 19/65 (29.2%) had a significant relapse. Compared with sustained clinical remission (SCR) + sustained response (SR) group, significant relapse group had a higher proportion of discontinued patients (47.4% <i>versus</i> 8.7%, <i>p</i> = 0.001). Among the 13 discontinued patients, the duration of maintenance therapy of the patients in significant relapse group was significantly shorter than that of the patients in SCR + SR group (months, median [IQR], 43.1 [32.0-62.4] <i>versus</i> 12.0 [5.1-22.0], <i>p</i> = 0.009). Multivariate logistic regression analysis showed that drug withdrawal was an independent risk factor for significant relapse [odds ratio (OR) = 10.4, confidence interval (CI) 95% 2.2-47.8, <i>p</i> = 0.003]. There was no significant difference between glucocorticoids (GCs) + hydroxychloroquine (HCQ) group and GCs + HCQ + immunosuppressive agents (ISAs) group in significant relapse rate (26.7% <i>versus</i> 22.2%, <i>p</i> > 0.05). The two SR curves of GCs + HCQ and GCs + HCQ+ ISA group basically coincided by the Cox regression analysis, demonstrating comparable long-term outcomes (<i>p</i> > 0.05).</p><p><strong>Conclusion: </strong>Drug withdrawal, especially abrupt withdrawal with insufficient duration of maintenance therapy, is an independent risk factor for significant relapse of SLE-ITP. HCQ combined with GCs is expected to be the first choice of the maintenance therapy for SLE-ITP patients.</p>","PeriodicalId":22960,"journal":{"name":"Therapeutic Advances in Chronic Disease","volume":"14 ","pages":"20406223231160688"},"PeriodicalIF":2.8000,"publicationDate":"2023-03-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/42/6d/10.1177_20406223231160688.PMC10031598.pdf","citationCount":"0","resultStr":"{\"title\":\"Risk factors of significant relapse and appropriate maintenance therapy strategy in SLE-associated immune thrombocytopenia.\",\"authors\":\"He-Jun Li, Yi-Qing Zheng, Ling Chen, Shun-Ping Lin, Xiang-Xiong Zheng\",\"doi\":\"10.1177/20406223231160688\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Systemic lupus erythematosus-associated immune thrombocytopenia (SLE-ITP) is characterized by relapse. The risk factors of relapse and appropriate maintenance therapy strategy deserve further exploration.</p><p><strong>Objectives: </strong>To determine the risk factors for relapse and appropriate maintenance therapy in significant SLE-ITP patients (a platelet count ⩽30 × 10<sup>9</sup>/l) after the first complete response.</p><p><strong>Design: </strong>Retrospective cohort study using the medical records of 105 patients diagnosed as significant SLE-ITP in Fujian Medical University Union Hospital during December 2012 to March 2021. Patients were followed through a call for observations in January 2022.</p><p><strong>Methods: </strong>Data including demographics, initial clinical feature, induction and maintenance therapy, and outcome at the end of follow-up were analyzed. Risk factors for significant relapse were analyzed using multivariate logistic regression models. The cumulative hazard of significant relapse and the duration of response were estimated, and the differences in outcome between groups were compared using the Cox regression analysis.</p><p><strong>Results: </strong>A total of 65 significant SLE-ITP patients were eligible for the final analysis. Median [interquartile range (IQR)] follow-up duration and median [IQR] duration of response were 62.2 [41.0-79.6] months and 43.4 [20.3-68.7] months, respectively. After the first complete response, 19/65 (29.2%) had a significant relapse. Compared with sustained clinical remission (SCR) + sustained response (SR) group, significant relapse group had a higher proportion of discontinued patients (47.4% <i>versus</i> 8.7%, <i>p</i> = 0.001). Among the 13 discontinued patients, the duration of maintenance therapy of the patients in significant relapse group was significantly shorter than that of the patients in SCR + SR group (months, median [IQR], 43.1 [32.0-62.4] <i>versus</i> 12.0 [5.1-22.0], <i>p</i> = 0.009). Multivariate logistic regression analysis showed that drug withdrawal was an independent risk factor for significant relapse [odds ratio (OR) = 10.4, confidence interval (CI) 95% 2.2-47.8, <i>p</i> = 0.003]. There was no significant difference between glucocorticoids (GCs) + hydroxychloroquine (HCQ) group and GCs + HCQ + immunosuppressive agents (ISAs) group in significant relapse rate (26.7% <i>versus</i> 22.2%, <i>p</i> > 0.05). The two SR curves of GCs + HCQ and GCs + HCQ+ ISA group basically coincided by the Cox regression analysis, demonstrating comparable long-term outcomes (<i>p</i> > 0.05).</p><p><strong>Conclusion: </strong>Drug withdrawal, especially abrupt withdrawal with insufficient duration of maintenance therapy, is an independent risk factor for significant relapse of SLE-ITP. HCQ combined with GCs is expected to be the first choice of the maintenance therapy for SLE-ITP patients.</p>\",\"PeriodicalId\":22960,\"journal\":{\"name\":\"Therapeutic Advances in Chronic Disease\",\"volume\":\"14 \",\"pages\":\"20406223231160688\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2023-03-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/42/6d/10.1177_20406223231160688.PMC10031598.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Chronic Disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/20406223231160688\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Chronic Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/20406223231160688","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Risk factors of significant relapse and appropriate maintenance therapy strategy in SLE-associated immune thrombocytopenia.
Background: Systemic lupus erythematosus-associated immune thrombocytopenia (SLE-ITP) is characterized by relapse. The risk factors of relapse and appropriate maintenance therapy strategy deserve further exploration.
Objectives: To determine the risk factors for relapse and appropriate maintenance therapy in significant SLE-ITP patients (a platelet count ⩽30 × 109/l) after the first complete response.
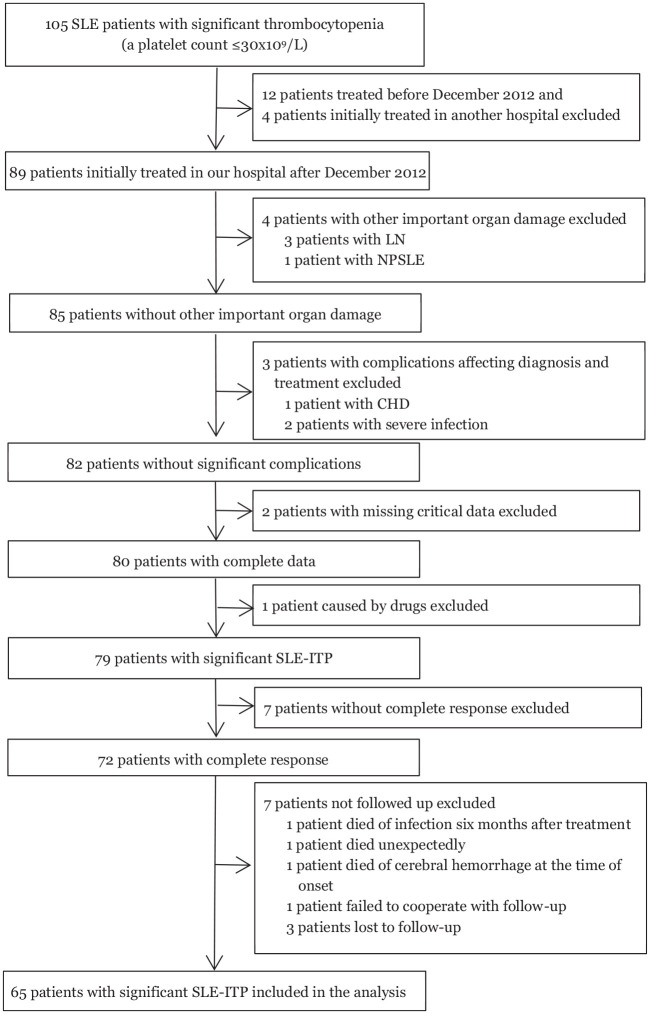
Design: Retrospective cohort study using the medical records of 105 patients diagnosed as significant SLE-ITP in Fujian Medical University Union Hospital during December 2012 to March 2021. Patients were followed through a call for observations in January 2022.
Methods: Data including demographics, initial clinical feature, induction and maintenance therapy, and outcome at the end of follow-up were analyzed. Risk factors for significant relapse were analyzed using multivariate logistic regression models. The cumulative hazard of significant relapse and the duration of response were estimated, and the differences in outcome between groups were compared using the Cox regression analysis.
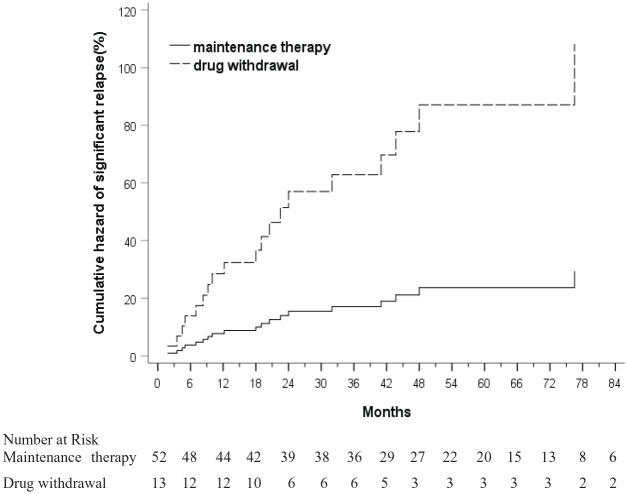
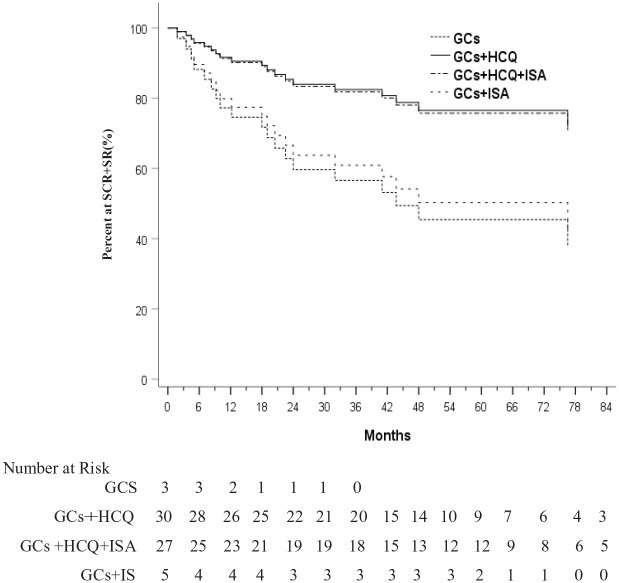
Results: A total of 65 significant SLE-ITP patients were eligible for the final analysis. Median [interquartile range (IQR)] follow-up duration and median [IQR] duration of response were 62.2 [41.0-79.6] months and 43.4 [20.3-68.7] months, respectively. After the first complete response, 19/65 (29.2%) had a significant relapse. Compared with sustained clinical remission (SCR) + sustained response (SR) group, significant relapse group had a higher proportion of discontinued patients (47.4% versus 8.7%, p = 0.001). Among the 13 discontinued patients, the duration of maintenance therapy of the patients in significant relapse group was significantly shorter than that of the patients in SCR + SR group (months, median [IQR], 43.1 [32.0-62.4] versus 12.0 [5.1-22.0], p = 0.009). Multivariate logistic regression analysis showed that drug withdrawal was an independent risk factor for significant relapse [odds ratio (OR) = 10.4, confidence interval (CI) 95% 2.2-47.8, p = 0.003]. There was no significant difference between glucocorticoids (GCs) + hydroxychloroquine (HCQ) group and GCs + HCQ + immunosuppressive agents (ISAs) group in significant relapse rate (26.7% versus 22.2%, p > 0.05). The two SR curves of GCs + HCQ and GCs + HCQ+ ISA group basically coincided by the Cox regression analysis, demonstrating comparable long-term outcomes (p > 0.05).
Conclusion: Drug withdrawal, especially abrupt withdrawal with insufficient duration of maintenance therapy, is an independent risk factor for significant relapse of SLE-ITP. HCQ combined with GCs is expected to be the first choice of the maintenance therapy for SLE-ITP patients.
期刊介绍:
Therapeutic Advances in Chronic Disease publishes the highest quality peer-reviewed research, reviews and scholarly comment in the drug treatment of all chronic diseases. The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers involved in the medical treatment of chronic disease, providing a forum in print and online for publishing the highest quality articles in this area.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
