Yaning Xu, Chengchun Liu, Wei Li, Ximing Nie, Shuhan Huang, Xiaoshu Li, Ya Wu, Wang-Sheng Jin, Jiaojin Jiang, Jun Dong, Yi Yang, Zhiqiang Sun, Wenjun Han, Yanjiang Wang, Liping Liu, Meng Zhang
{"title":"心房颤动患者血管内治疗后早期抗凝的有效性和安全性。","authors":"Yaning Xu, Chengchun Liu, Wei Li, Ximing Nie, Shuhan Huang, Xiaoshu Li, Ya Wu, Wang-Sheng Jin, Jiaojin Jiang, Jun Dong, Yi Yang, Zhiqiang Sun, Wenjun Han, Yanjiang Wang, Liping Liu, Meng Zhang","doi":"10.1136/svn-2022-002082","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The timing for initiating anticoagulant therapy in acute ischaemic stroke (AIS) patients with atrial fibrillation who recanalised after endovascular treatment (EVT) is unclear. The objective of this study was to evaluate the effect of early anticoagulation after successful recanalisation in AIS patients with atrial fibrillation.</p><p><strong>Methods: </strong>Patients with anterior circulation large vessel occlusion and atrial fibrillation who were successfully recanalised by EVT within 24 hours after stroke in the Registration Study for Critical Care of Acute Ischemic Stroke after Recanalization registry were analysed. Early anticoagulation was defined as the initiation of unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) within 72 hours after EVT. Ultra-early anticoagulation was defined if it was initiated within 24 hours. The primary efficacy outcome was the score on the modified Rankin Scale (mRS) at day 90, and the primary safety outcome was symptomatic intracranial haemorrhage within 90 days.</p><p><strong>Results: </strong>Overall, 257 patients were enrolled, of whom 141 (54.9%) initiated anticoagulation within 72 hours after EVT, including 111 within 24 hours. A significant shift towards better mRS scores at day 90 was associated with early anticoagulation (adjusted common OR 2.08 (95% CI 1.27 to 3.41)). Symptomatic intracranial haemorrhage was comparable between patients treated with early and routine anticoagulation (adjusted OR 0.20 (95% CI 0.02 to 2.18)). Comparison of different early anticoagulation regimens showed that ultra-early anticoagulation was more significantly associated with favourable functional outcomes (adjusted common OR 2.03 (95% CI 1.20 to 3.44)) and reduced the incidence of asymptomatic intracranial haemorrhage (OR 0.37 (95% CI 0.14 to 0.94)).</p><p><strong>Conclusions: </strong>In AIS patients with atrial fibrillation, early anticoagulation with UFH or LMWH after successful recanalisation is associated with favourable functional outcomes without increasing the risk of symptomatic intracranial haemorrhages.</p><p><strong>Trial registration number: </strong>ChiCTR1900022154.</p>","PeriodicalId":22021,"journal":{"name":"Stroke and Vascular Neurology","volume":" ","pages":"405-412"},"PeriodicalIF":4.9000,"publicationDate":"2023-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10647876/pdf/","citationCount":"0","resultStr":"{\"title\":\"Efficacy and safety of early anticoagulation after endovascular treatment in patients with atrial fibrillation.\",\"authors\":\"Yaning Xu, Chengchun Liu, Wei Li, Ximing Nie, Shuhan Huang, Xiaoshu Li, Ya Wu, Wang-Sheng Jin, Jiaojin Jiang, Jun Dong, Yi Yang, Zhiqiang Sun, Wenjun Han, Yanjiang Wang, Liping Liu, Meng Zhang\",\"doi\":\"10.1136/svn-2022-002082\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The timing for initiating anticoagulant therapy in acute ischaemic stroke (AIS) patients with atrial fibrillation who recanalised after endovascular treatment (EVT) is unclear. The objective of this study was to evaluate the effect of early anticoagulation after successful recanalisation in AIS patients with atrial fibrillation.</p><p><strong>Methods: </strong>Patients with anterior circulation large vessel occlusion and atrial fibrillation who were successfully recanalised by EVT within 24 hours after stroke in the Registration Study for Critical Care of Acute Ischemic Stroke after Recanalization registry were analysed. Early anticoagulation was defined as the initiation of unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) within 72 hours after EVT. Ultra-early anticoagulation was defined if it was initiated within 24 hours. The primary efficacy outcome was the score on the modified Rankin Scale (mRS) at day 90, and the primary safety outcome was symptomatic intracranial haemorrhage within 90 days.</p><p><strong>Results: </strong>Overall, 257 patients were enrolled, of whom 141 (54.9%) initiated anticoagulation within 72 hours after EVT, including 111 within 24 hours. A significant shift towards better mRS scores at day 90 was associated with early anticoagulation (adjusted common OR 2.08 (95% CI 1.27 to 3.41)). Symptomatic intracranial haemorrhage was comparable between patients treated with early and routine anticoagulation (adjusted OR 0.20 (95% CI 0.02 to 2.18)). Comparison of different early anticoagulation regimens showed that ultra-early anticoagulation was more significantly associated with favourable functional outcomes (adjusted common OR 2.03 (95% CI 1.20 to 3.44)) and reduced the incidence of asymptomatic intracranial haemorrhage (OR 0.37 (95% CI 0.14 to 0.94)).</p><p><strong>Conclusions: </strong>In AIS patients with atrial fibrillation, early anticoagulation with UFH or LMWH after successful recanalisation is associated with favourable functional outcomes without increasing the risk of symptomatic intracranial haemorrhages.</p><p><strong>Trial registration number: </strong>ChiCTR1900022154.</p>\",\"PeriodicalId\":22021,\"journal\":{\"name\":\"Stroke and Vascular Neurology\",\"volume\":\" \",\"pages\":\"405-412\"},\"PeriodicalIF\":4.9000,\"publicationDate\":\"2023-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10647876/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Stroke and Vascular Neurology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/svn-2022-002082\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/3/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stroke and Vascular Neurology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/svn-2022-002082","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/3/27 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Efficacy and safety of early anticoagulation after endovascular treatment in patients with atrial fibrillation.
Background: The timing for initiating anticoagulant therapy in acute ischaemic stroke (AIS) patients with atrial fibrillation who recanalised after endovascular treatment (EVT) is unclear. The objective of this study was to evaluate the effect of early anticoagulation after successful recanalisation in AIS patients with atrial fibrillation.
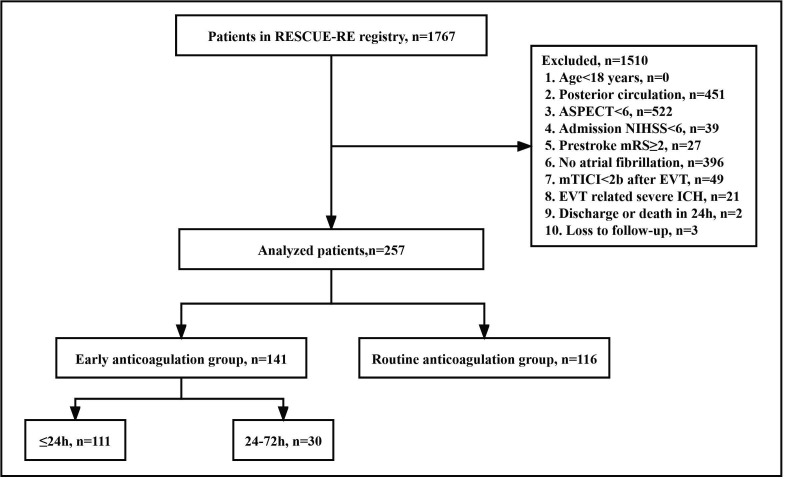
Methods: Patients with anterior circulation large vessel occlusion and atrial fibrillation who were successfully recanalised by EVT within 24 hours after stroke in the Registration Study for Critical Care of Acute Ischemic Stroke after Recanalization registry were analysed. Early anticoagulation was defined as the initiation of unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) within 72 hours after EVT. Ultra-early anticoagulation was defined if it was initiated within 24 hours. The primary efficacy outcome was the score on the modified Rankin Scale (mRS) at day 90, and the primary safety outcome was symptomatic intracranial haemorrhage within 90 days.
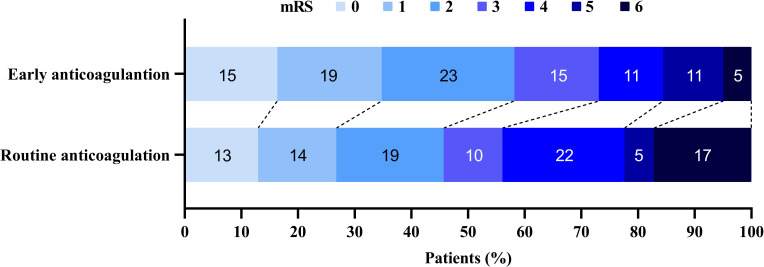
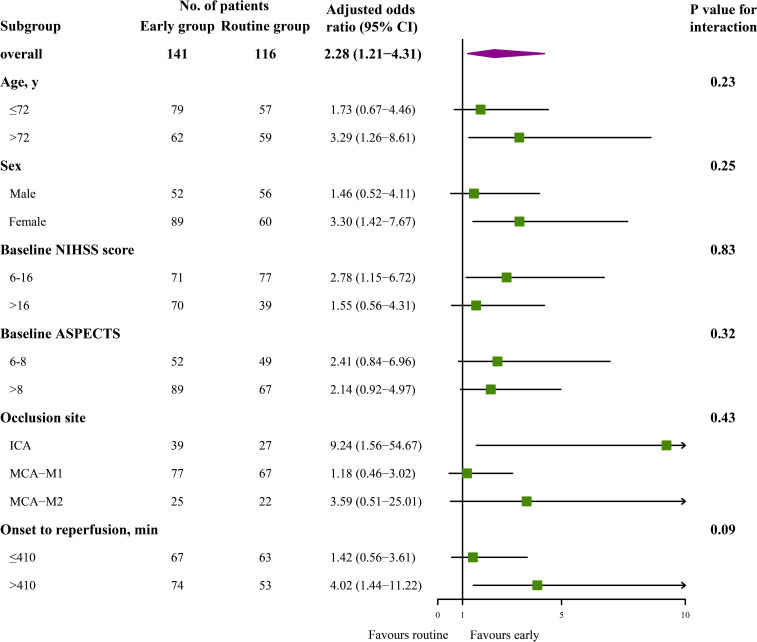
Results: Overall, 257 patients were enrolled, of whom 141 (54.9%) initiated anticoagulation within 72 hours after EVT, including 111 within 24 hours. A significant shift towards better mRS scores at day 90 was associated with early anticoagulation (adjusted common OR 2.08 (95% CI 1.27 to 3.41)). Symptomatic intracranial haemorrhage was comparable between patients treated with early and routine anticoagulation (adjusted OR 0.20 (95% CI 0.02 to 2.18)). Comparison of different early anticoagulation regimens showed that ultra-early anticoagulation was more significantly associated with favourable functional outcomes (adjusted common OR 2.03 (95% CI 1.20 to 3.44)) and reduced the incidence of asymptomatic intracranial haemorrhage (OR 0.37 (95% CI 0.14 to 0.94)).
Conclusions: In AIS patients with atrial fibrillation, early anticoagulation with UFH or LMWH after successful recanalisation is associated with favourable functional outcomes without increasing the risk of symptomatic intracranial haemorrhages.
期刊介绍:
Stroke and Vascular Neurology (SVN) is the official journal of the Chinese Stroke Association. Supported by a team of renowned Editors, and fully Open Access, the journal encourages debate on controversial techniques, issues on health policy and social medicine.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
