Antonio Pellegrino, Mario Villa, Maria Cristina Cesana, Anna Myriam Perrone, Antonio Malvasi, Vera Loizzi, Pierluigi Giampaolino, Ettore Cicinelli, Pierandrea De Iaco, Gianluca Raffaello Damiani
{"title":"机器人侧盆腔器官脱垂多室阴道脱垂悬吊。","authors":"Antonio Pellegrino, Mario Villa, Maria Cristina Cesana, Anna Myriam Perrone, Antonio Malvasi, Vera Loizzi, Pierluigi Giampaolino, Ettore Cicinelli, Pierandrea De Iaco, Gianluca Raffaello Damiani","doi":"10.4103/gmit.gmit_97_21","DOIUrl":null,"url":null,"abstract":"InteRventIons The procedure uses a titanized propylene prosthesis shaped in T that gives it maneuverability and elasticity proper to native tissues. The positioning technique involves a first phase of removing peritoneum from the vaginal dome and then the disconnect of the vescicovaginal band to delimit the mesh anchoring plans. The lateral trajectory of it consists to insert in a retrograde manner the side arm of the prothesis in the context of the lateral abdominal wall with a posterior projection to the anterior-upper iliac crest in a space which is free of major complications [Figures 1 and 2]. Procedure started with dissection of the cervicovesical pouch. The vesicovaginal space was then identified between the bladder and the anterior vaginal wall. A mesh (Endolas® 41.5 cm × 5 cm × 15 cm) with two lateral arms was tailored and fixed to the vagina, by six sutures of 2-0 polyglactin 910. The","PeriodicalId":45272,"journal":{"name":"Gynecology and Minimally Invasive Therapy-GMIT","volume":"12 1","pages":"44-45"},"PeriodicalIF":2.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3f/85/GMIT-12-44.PMC10071865.pdf","citationCount":"2","resultStr":"{\"title\":\"Robotic Lateral Pelvic Organ Prolapse Suspension of Multicompartment Vaginal Prolapse.\",\"authors\":\"Antonio Pellegrino, Mario Villa, Maria Cristina Cesana, Anna Myriam Perrone, Antonio Malvasi, Vera Loizzi, Pierluigi Giampaolino, Ettore Cicinelli, Pierandrea De Iaco, Gianluca Raffaello Damiani\",\"doi\":\"10.4103/gmit.gmit_97_21\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"InteRventIons The procedure uses a titanized propylene prosthesis shaped in T that gives it maneuverability and elasticity proper to native tissues. The positioning technique involves a first phase of removing peritoneum from the vaginal dome and then the disconnect of the vescicovaginal band to delimit the mesh anchoring plans. The lateral trajectory of it consists to insert in a retrograde manner the side arm of the prothesis in the context of the lateral abdominal wall with a posterior projection to the anterior-upper iliac crest in a space which is free of major complications [Figures 1 and 2]. Procedure started with dissection of the cervicovesical pouch. The vesicovaginal space was then identified between the bladder and the anterior vaginal wall. A mesh (Endolas® 41.5 cm × 5 cm × 15 cm) with two lateral arms was tailored and fixed to the vagina, by six sutures of 2-0 polyglactin 910. The\",\"PeriodicalId\":45272,\"journal\":{\"name\":\"Gynecology and Minimally Invasive Therapy-GMIT\",\"volume\":\"12 1\",\"pages\":\"44-45\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3f/85/GMIT-12-44.PMC10071865.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gynecology and Minimally Invasive Therapy-GMIT\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/gmit.gmit_97_21\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gynecology and Minimally Invasive Therapy-GMIT","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/gmit.gmit_97_21","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Robotic Lateral Pelvic Organ Prolapse Suspension of Multicompartment Vaginal Prolapse.
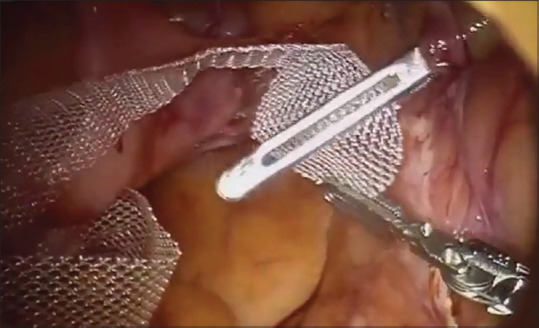
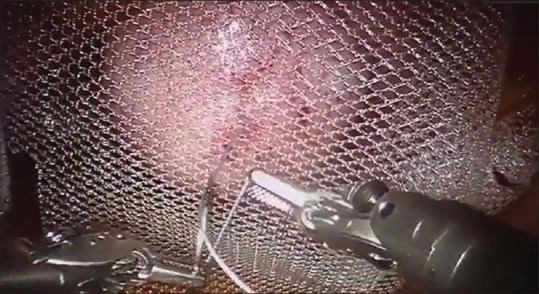
InteRventIons The procedure uses a titanized propylene prosthesis shaped in T that gives it maneuverability and elasticity proper to native tissues. The positioning technique involves a first phase of removing peritoneum from the vaginal dome and then the disconnect of the vescicovaginal band to delimit the mesh anchoring plans. The lateral trajectory of it consists to insert in a retrograde manner the side arm of the prothesis in the context of the lateral abdominal wall with a posterior projection to the anterior-upper iliac crest in a space which is free of major complications [Figures 1 and 2]. Procedure started with dissection of the cervicovesical pouch. The vesicovaginal space was then identified between the bladder and the anterior vaginal wall. A mesh (Endolas® 41.5 cm × 5 cm × 15 cm) with two lateral arms was tailored and fixed to the vagina, by six sutures of 2-0 polyglactin 910. The




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
