Nazife Şule Yaşar Bilge, Sultan Özkurt, Mustafa Fuat Açıkalın, Timuçin Kaşifoğlu
{"title":"微小变化疾病和原发性干燥综合征并发:基于病例的回顾。","authors":"Nazife Şule Yaşar Bilge, Sultan Özkurt, Mustafa Fuat Açıkalın, Timuçin Kaşifoğlu","doi":"10.5152/eurjrheum.2022.20246","DOIUrl":null,"url":null,"abstract":"<p><p>Primary Sjogren's syndrome is a chronic autoimmune disease with glandular and extraglandular features. Renal involvement is less frequent when compared with other systemic manifestations. Glomerulonephritis is a relatively rare manifestation of primary Sjogren's syndrome. Among all types of glomerular manifestations, minimal change disease is rarely identified, and there are only a few cases in the literature. Herein, we present a 53-year-old male patient who was diagnosed with primary Sjogren's syndrome and minimal change disease while searching for the etiopathogenesis of nephrotic syndrome. The patient had edema, dyspnea, hypertension, and 12 g/day proteinuria at admission. Serum albumin level was 1.82 g/dL, and renal function tests were within normal ranges. Renal biopsy findings were consistent with minimal change disease. At the same time, he was diagnosed with primary Sjogren's syndrome based on dry eyes demonstrated with Schirmer's test, positive antinuclear antibody, anti-SS-A, and anti-SS-B antibodies. Hydroxychloroquine with methylprednisolone 1 mg/kg (64 mg/day) was started, and methylprednisolone was slowly tapered. His proteinuria regressed to 79.2 mg/day, creatinine level was 0.83 mg/dL, and serum albumin level increased to 3.88 g/dL on the second week of the glucocorticoid treatment. In this case-based review, we present our case with 5 other reports of minimal change disease associated with primary Sjogren's syndrome. Our aim was to increase the awareness of this rare concurrence both among rheumatologists and nephrologists in light of the literature review.</p>","PeriodicalId":12066,"journal":{"name":"European journal of rheumatology","volume":"9 4","pages":"221-224"},"PeriodicalIF":1.8000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5a/b8/ejr-9-4-221.PMC10089134.pdf","citationCount":"1","resultStr":"{\"title\":\"Minimal Change Disease and Primary Sjogren Syndrome Concurrence: Case-Based review.\",\"authors\":\"Nazife Şule Yaşar Bilge, Sultan Özkurt, Mustafa Fuat Açıkalın, Timuçin Kaşifoğlu\",\"doi\":\"10.5152/eurjrheum.2022.20246\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Primary Sjogren's syndrome is a chronic autoimmune disease with glandular and extraglandular features. Renal involvement is less frequent when compared with other systemic manifestations. Glomerulonephritis is a relatively rare manifestation of primary Sjogren's syndrome. Among all types of glomerular manifestations, minimal change disease is rarely identified, and there are only a few cases in the literature. Herein, we present a 53-year-old male patient who was diagnosed with primary Sjogren's syndrome and minimal change disease while searching for the etiopathogenesis of nephrotic syndrome. The patient had edema, dyspnea, hypertension, and 12 g/day proteinuria at admission. Serum albumin level was 1.82 g/dL, and renal function tests were within normal ranges. Renal biopsy findings were consistent with minimal change disease. At the same time, he was diagnosed with primary Sjogren's syndrome based on dry eyes demonstrated with Schirmer's test, positive antinuclear antibody, anti-SS-A, and anti-SS-B antibodies. Hydroxychloroquine with methylprednisolone 1 mg/kg (64 mg/day) was started, and methylprednisolone was slowly tapered. His proteinuria regressed to 79.2 mg/day, creatinine level was 0.83 mg/dL, and serum albumin level increased to 3.88 g/dL on the second week of the glucocorticoid treatment. In this case-based review, we present our case with 5 other reports of minimal change disease associated with primary Sjogren's syndrome. Our aim was to increase the awareness of this rare concurrence both among rheumatologists and nephrologists in light of the literature review.</p>\",\"PeriodicalId\":12066,\"journal\":{\"name\":\"European journal of rheumatology\",\"volume\":\"9 4\",\"pages\":\"221-224\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2022-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5a/b8/ejr-9-4-221.PMC10089134.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European journal of rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5152/eurjrheum.2022.20246\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5152/eurjrheum.2022.20246","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
Minimal Change Disease and Primary Sjogren Syndrome Concurrence: Case-Based review.
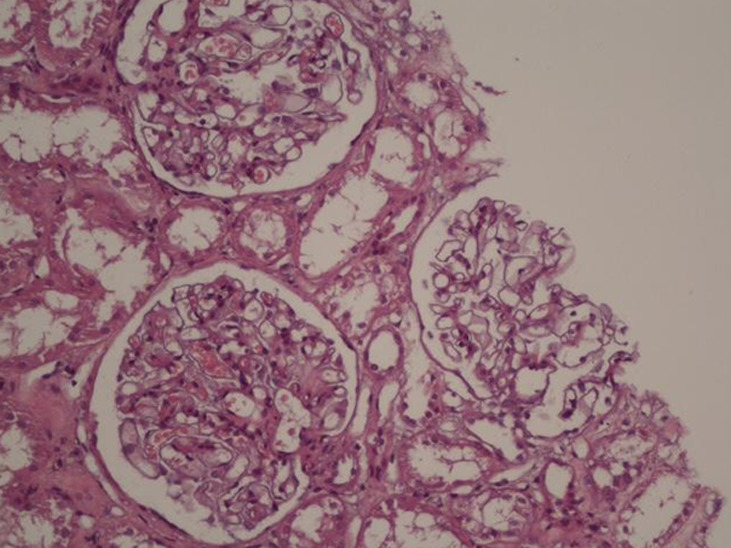
Primary Sjogren's syndrome is a chronic autoimmune disease with glandular and extraglandular features. Renal involvement is less frequent when compared with other systemic manifestations. Glomerulonephritis is a relatively rare manifestation of primary Sjogren's syndrome. Among all types of glomerular manifestations, minimal change disease is rarely identified, and there are only a few cases in the literature. Herein, we present a 53-year-old male patient who was diagnosed with primary Sjogren's syndrome and minimal change disease while searching for the etiopathogenesis of nephrotic syndrome. The patient had edema, dyspnea, hypertension, and 12 g/day proteinuria at admission. Serum albumin level was 1.82 g/dL, and renal function tests were within normal ranges. Renal biopsy findings were consistent with minimal change disease. At the same time, he was diagnosed with primary Sjogren's syndrome based on dry eyes demonstrated with Schirmer's test, positive antinuclear antibody, anti-SS-A, and anti-SS-B antibodies. Hydroxychloroquine with methylprednisolone 1 mg/kg (64 mg/day) was started, and methylprednisolone was slowly tapered. His proteinuria regressed to 79.2 mg/day, creatinine level was 0.83 mg/dL, and serum albumin level increased to 3.88 g/dL on the second week of the glucocorticoid treatment. In this case-based review, we present our case with 5 other reports of minimal change disease associated with primary Sjogren's syndrome. Our aim was to increase the awareness of this rare concurrence both among rheumatologists and nephrologists in light of the literature review.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
