Ishaq M Alkooheji, Mohamed Alabbasi, Shehab Khashaba, Mohamed A M Ebrahim Rafie, Martin Corbally
{"title":"巴林一所大学医院睾丸扭转患者的回顾性分析。","authors":"Ishaq M Alkooheji, Mohamed Alabbasi, Shehab Khashaba, Mohamed A M Ebrahim Rafie, Martin Corbally","doi":"10.4103/ua.ua_107_22","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Testicular torsion is a surgical emergency that, with delayed treatment, may be associated with loss of the testis. It commonly presents with sudden onset testicular pain, vague lower abdominal pain, nausea, and vomiting. Management often requires emergent surgical scrotal exploration, detorsion, and fixation or removal of the affected testis.</p><p><strong>Materials and methods: </strong>Retrospective review of all the patients in a hospital covering the Muharraq district in Bahrain presenting with testicular pain.</p><p><strong>Results: </strong>During the six-year period from 2015 to 2021, 48 patients with testicular torsion were managed, with a mean age of 18.4 (± 9.2) years. Most patients (54.7%) presented within 6 hours of the onset of symptoms. All 48 patients underwent a doppler ultrasound, which confirmed the presence of testicular torsion in 87.5% of patients, with a sensitivity of 87% and specificity of 98.5%. Fourteen patients had non-viable testis on surgical exploration, with an average age of 16.6 (± 6.8) years and took an average of 13 to 24 hours to present to the emergency department after the start of pain. Most patients underwent scrotal ultrasound 60 minutes from the presentation to the emergency department and surgical exploration within 120 to 179 minutes. The rate of testicular torsion in patients who underwent diagnostic ultrasound at 60 minutes or more from presentation was 40%, compared to an overall rate of 29%. All detected cases of testicular torsion, except for one case, underwent bilateral fixation of the testes. Of those patients who underwent contralateral fixation, none presented with contralateral torsion, supporting the recommendation of contralateral fixation.</p><p><strong>Conclusion: </strong>Patients underwent comprehensive assessment of their complaint and emergent surgical intervention, including an ultrasound that did not delay the surgical intervention. We agree that clinical judgment is the primary tool for assessment of patients with acute scrotum and an adjunct emergent ultrasound does not significantly cause delays. We concur with the current recommendations for contralateral fixation and prompt surgical management as the anatomical anomaly is present bilaterally.</p>","PeriodicalId":23633,"journal":{"name":"Urology Annals","volume":"15 1","pages":"8-14"},"PeriodicalIF":0.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a7/4c/UA-15-8.PMC10062518.pdf","citationCount":"0","resultStr":"{\"title\":\"Retrospective review of patients with testicular torsion in a University Hospital in Bahrain.\",\"authors\":\"Ishaq M Alkooheji, Mohamed Alabbasi, Shehab Khashaba, Mohamed A M Ebrahim Rafie, Martin Corbally\",\"doi\":\"10.4103/ua.ua_107_22\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Testicular torsion is a surgical emergency that, with delayed treatment, may be associated with loss of the testis. It commonly presents with sudden onset testicular pain, vague lower abdominal pain, nausea, and vomiting. Management often requires emergent surgical scrotal exploration, detorsion, and fixation or removal of the affected testis.</p><p><strong>Materials and methods: </strong>Retrospective review of all the patients in a hospital covering the Muharraq district in Bahrain presenting with testicular pain.</p><p><strong>Results: </strong>During the six-year period from 2015 to 2021, 48 patients with testicular torsion were managed, with a mean age of 18.4 (± 9.2) years. Most patients (54.7%) presented within 6 hours of the onset of symptoms. All 48 patients underwent a doppler ultrasound, which confirmed the presence of testicular torsion in 87.5% of patients, with a sensitivity of 87% and specificity of 98.5%. Fourteen patients had non-viable testis on surgical exploration, with an average age of 16.6 (± 6.8) years and took an average of 13 to 24 hours to present to the emergency department after the start of pain. Most patients underwent scrotal ultrasound 60 minutes from the presentation to the emergency department and surgical exploration within 120 to 179 minutes. The rate of testicular torsion in patients who underwent diagnostic ultrasound at 60 minutes or more from presentation was 40%, compared to an overall rate of 29%. All detected cases of testicular torsion, except for one case, underwent bilateral fixation of the testes. Of those patients who underwent contralateral fixation, none presented with contralateral torsion, supporting the recommendation of contralateral fixation.</p><p><strong>Conclusion: </strong>Patients underwent comprehensive assessment of their complaint and emergent surgical intervention, including an ultrasound that did not delay the surgical intervention. We agree that clinical judgment is the primary tool for assessment of patients with acute scrotum and an adjunct emergent ultrasound does not significantly cause delays. We concur with the current recommendations for contralateral fixation and prompt surgical management as the anatomical anomaly is present bilaterally.</p>\",\"PeriodicalId\":23633,\"journal\":{\"name\":\"Urology Annals\",\"volume\":\"15 1\",\"pages\":\"8-14\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a7/4c/UA-15-8.PMC10062518.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Urology Annals\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/ua.ua_107_22\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/17 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Urology Annals","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/ua.ua_107_22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/17 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Retrospective review of patients with testicular torsion in a University Hospital in Bahrain.
Introduction: Testicular torsion is a surgical emergency that, with delayed treatment, may be associated with loss of the testis. It commonly presents with sudden onset testicular pain, vague lower abdominal pain, nausea, and vomiting. Management often requires emergent surgical scrotal exploration, detorsion, and fixation or removal of the affected testis.
Materials and methods: Retrospective review of all the patients in a hospital covering the Muharraq district in Bahrain presenting with testicular pain.
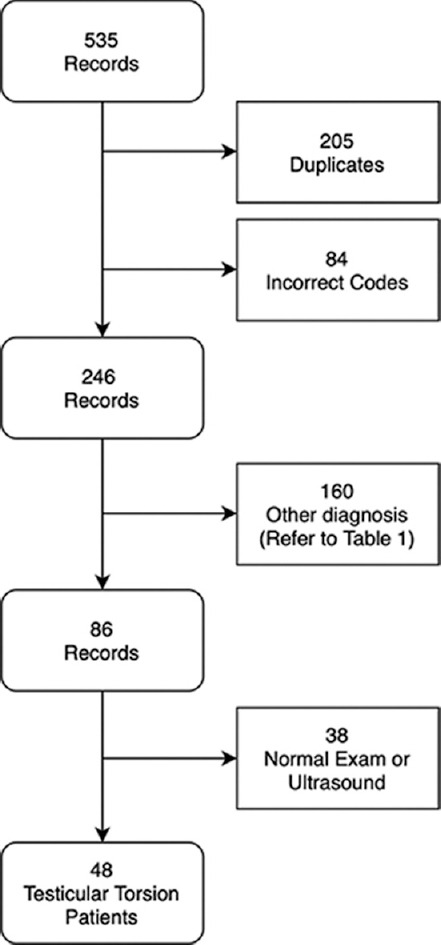
Results: During the six-year period from 2015 to 2021, 48 patients with testicular torsion were managed, with a mean age of 18.4 (± 9.2) years. Most patients (54.7%) presented within 6 hours of the onset of symptoms. All 48 patients underwent a doppler ultrasound, which confirmed the presence of testicular torsion in 87.5% of patients, with a sensitivity of 87% and specificity of 98.5%. Fourteen patients had non-viable testis on surgical exploration, with an average age of 16.6 (± 6.8) years and took an average of 13 to 24 hours to present to the emergency department after the start of pain. Most patients underwent scrotal ultrasound 60 minutes from the presentation to the emergency department and surgical exploration within 120 to 179 minutes. The rate of testicular torsion in patients who underwent diagnostic ultrasound at 60 minutes or more from presentation was 40%, compared to an overall rate of 29%. All detected cases of testicular torsion, except for one case, underwent bilateral fixation of the testes. Of those patients who underwent contralateral fixation, none presented with contralateral torsion, supporting the recommendation of contralateral fixation.
Conclusion: Patients underwent comprehensive assessment of their complaint and emergent surgical intervention, including an ultrasound that did not delay the surgical intervention. We agree that clinical judgment is the primary tool for assessment of patients with acute scrotum and an adjunct emergent ultrasound does not significantly cause delays. We concur with the current recommendations for contralateral fixation and prompt surgical management as the anatomical anomaly is present bilaterally.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
