A V Vitebskaya, Ekaterina S Bugakova, E A Pisareva, Yu V Tikhonovich
{"title":"[输血依赖性遗传性贫血患者的内分泌紊乱]。","authors":"A V Vitebskaya, Ekaterina S Bugakova, E A Pisareva, Yu V Tikhonovich","doi":"10.14341/probl13149","DOIUrl":null,"url":null,"abstract":"<p><p>Often transfusions red blood cells in patients with hereditary anemias lead to iron overload, that can cause endocrine complications, such as growth retardation, hypothyroidism, hypogonadism, and disorders of carbohydrate metabolism.Clinical case 1. A boy with transfusion-dependent (TD) Diamond-Blackfan anemia at 16.3 years presented with impaired fasting glucose, growth hormone (GH) deficiency, hypogonadotropic hypogonadism; GH therapy was initiated. At the age of 16.8 years old secondary hypothyroidism, secondary hypocorticism and diabetes mellitus were diagnosed. At 17.2 years continuous glucose monitoring (CGM) detected glucose elevations up to 11.7 mmol/l. Therapy with GH and testosterone ethers was continued; levothyroxine and cortef were stopped by patient. At 17.9 years height was 163 cm; no data supporting hypothyroidism nor hypocorticism; glycaemia within goal range.Clinical case 2. A girl with TD beta-thalassemia major at the age of 11.5 years presented with GH deficiency; GH therapy has been conducted from 12.8 to 15.3 years of age. At 13.8 years retardation of pubertal development was diagnosed. At 15.0 hyperglycemia 7.2 mmol/l was detected; normal results of oral glucose tolerance test (OGTT) were observed; glycemia elevations were up to 9.5 mmol/l according to CGM data. At 16.0 height was 152 cm; because of pubertal development arrest hormone replacement therapy was prescribed.CONCLUSION. Growth, pubertal and carbohydrate metabolism disorders were diagnosed in patients with TD hereditary anemias, that confirms the necessity of regularly endocrine investigation. To detect impairment of carbohydrate metabolism investigation of fasting blood glucose, OGTT, and CGM is recommended; glycated hemoglobin measurement is not considered reasonable.</p>","PeriodicalId":20433,"journal":{"name":"Problemy endokrinologii","volume":"68 6","pages":"121-130"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9939971/pdf/","citationCount":"0","resultStr":"{\"title\":\"[Endocrine disorders in patients with transfusion-dependent hereditary anemias].\",\"authors\":\"A V Vitebskaya, Ekaterina S Bugakova, E A Pisareva, Yu V Tikhonovich\",\"doi\":\"10.14341/probl13149\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Often transfusions red blood cells in patients with hereditary anemias lead to iron overload, that can cause endocrine complications, such as growth retardation, hypothyroidism, hypogonadism, and disorders of carbohydrate metabolism.Clinical case 1. A boy with transfusion-dependent (TD) Diamond-Blackfan anemia at 16.3 years presented with impaired fasting glucose, growth hormone (GH) deficiency, hypogonadotropic hypogonadism; GH therapy was initiated. At the age of 16.8 years old secondary hypothyroidism, secondary hypocorticism and diabetes mellitus were diagnosed. At 17.2 years continuous glucose monitoring (CGM) detected glucose elevations up to 11.7 mmol/l. Therapy with GH and testosterone ethers was continued; levothyroxine and cortef were stopped by patient. At 17.9 years height was 163 cm; no data supporting hypothyroidism nor hypocorticism; glycaemia within goal range.Clinical case 2. A girl with TD beta-thalassemia major at the age of 11.5 years presented with GH deficiency; GH therapy has been conducted from 12.8 to 15.3 years of age. At 13.8 years retardation of pubertal development was diagnosed. At 15.0 hyperglycemia 7.2 mmol/l was detected; normal results of oral glucose tolerance test (OGTT) were observed; glycemia elevations were up to 9.5 mmol/l according to CGM data. At 16.0 height was 152 cm; because of pubertal development arrest hormone replacement therapy was prescribed.CONCLUSION. Growth, pubertal and carbohydrate metabolism disorders were diagnosed in patients with TD hereditary anemias, that confirms the necessity of regularly endocrine investigation. To detect impairment of carbohydrate metabolism investigation of fasting blood glucose, OGTT, and CGM is recommended; glycated hemoglobin measurement is not considered reasonable.</p>\",\"PeriodicalId\":20433,\"journal\":{\"name\":\"Problemy endokrinologii\",\"volume\":\"68 6\",\"pages\":\"121-130\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-07-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9939971/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Problemy endokrinologii\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14341/probl13149\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Problemy endokrinologii","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14341/probl13149","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
[Endocrine disorders in patients with transfusion-dependent hereditary anemias].
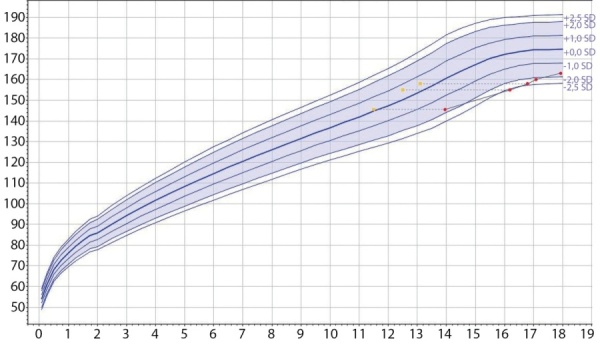
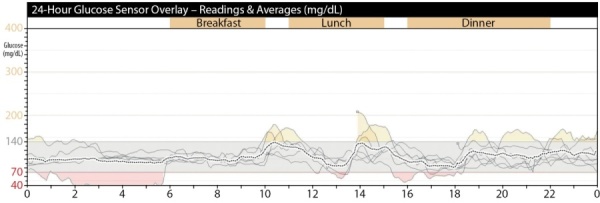
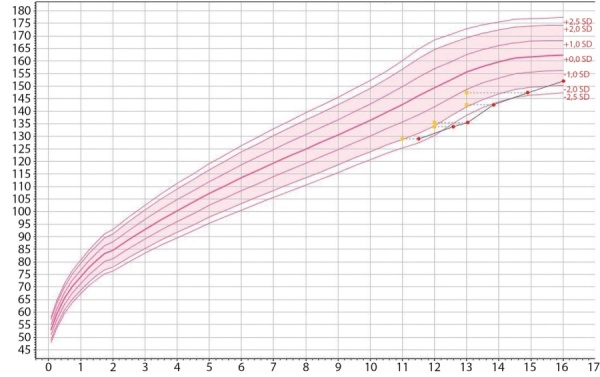
Often transfusions red blood cells in patients with hereditary anemias lead to iron overload, that can cause endocrine complications, such as growth retardation, hypothyroidism, hypogonadism, and disorders of carbohydrate metabolism.Clinical case 1. A boy with transfusion-dependent (TD) Diamond-Blackfan anemia at 16.3 years presented with impaired fasting glucose, growth hormone (GH) deficiency, hypogonadotropic hypogonadism; GH therapy was initiated. At the age of 16.8 years old secondary hypothyroidism, secondary hypocorticism and diabetes mellitus were diagnosed. At 17.2 years continuous glucose monitoring (CGM) detected glucose elevations up to 11.7 mmol/l. Therapy with GH and testosterone ethers was continued; levothyroxine and cortef were stopped by patient. At 17.9 years height was 163 cm; no data supporting hypothyroidism nor hypocorticism; glycaemia within goal range.Clinical case 2. A girl with TD beta-thalassemia major at the age of 11.5 years presented with GH deficiency; GH therapy has been conducted from 12.8 to 15.3 years of age. At 13.8 years retardation of pubertal development was diagnosed. At 15.0 hyperglycemia 7.2 mmol/l was detected; normal results of oral glucose tolerance test (OGTT) were observed; glycemia elevations were up to 9.5 mmol/l according to CGM data. At 16.0 height was 152 cm; because of pubertal development arrest hormone replacement therapy was prescribed.CONCLUSION. Growth, pubertal and carbohydrate metabolism disorders were diagnosed in patients with TD hereditary anemias, that confirms the necessity of regularly endocrine investigation. To detect impairment of carbohydrate metabolism investigation of fasting blood glucose, OGTT, and CGM is recommended; glycated hemoglobin measurement is not considered reasonable.
期刊介绍:
Since 1955 the “Problems of Endocrinology” (or “Problemy Endocrinologii”) Journal publishes timely articles, balancing both clinical and experimental research, case reports, reviews and lectures on pressing problems of endocrinology. The Journal is aimed to the most topical issues of endocrinology: to chemical structure, biosynthesis and metabolism of hormones, the mechanism of their action at cellular and molecular level; pathogenesis and to clinic of the endocrine diseases, new methods of their diagnostics and treatment. The Journal: features original national and foreign research articles, reflecting world endocrinology development; issues thematic editions on specific areas; publishes chronicle of major international congress sessions and workshops on endocrinology, as well as state-of-the-art guidelines; is intended for scientists, endocrinologists diabetologists and specialists of allied trade, general practitioners, family physicians and pediatrics.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
