Elizabeth A Mosley, Sequoia Ayala, Zainab Jah, Tiffany Hailstorks, Indya Hairston, Whitney S Rice, Natalie Hernandez, Kwajelyn Jackson, Marieh Scales, Mariana Gutierrez, Bria Goode, Sofia Filippa, Shani Strader, Mariana Umbria, Autumn Watson, Joya Faruque, Adeola Raji, Janae Dunkley, Peyton Rogers, Celeste Ellison, Kheyanna Suarez, Dázon Dixon Diallo, Kelli S Hall
{"title":"“我一点也不后悔。只是我希望这个过程更人性化一点……更全面一点”:一项定性的、社区主导的药物流产研究,研究对象是美国佐治亚州的黑人和拉丁裔妇女。","authors":"Elizabeth A Mosley, Sequoia Ayala, Zainab Jah, Tiffany Hailstorks, Indya Hairston, Whitney S Rice, Natalie Hernandez, Kwajelyn Jackson, Marieh Scales, Mariana Gutierrez, Bria Goode, Sofia Filippa, Shani Strader, Mariana Umbria, Autumn Watson, Joya Faruque, Adeola Raji, Janae Dunkley, Peyton Rogers, Celeste Ellison, Kheyanna Suarez, Dázon Dixon Diallo, Kelli S Hall","doi":"10.1080/26410397.2022.2129686","DOIUrl":null,"url":null,"abstract":"<p><p>Traditional family planning research has excluded Black and Latinx leaders, and little is known about medication abortion (MA) among racial/ethnic minorities, although it is an increasingly vital reproductive health service, particularly after the fall of <i>Roe v. Wade</i>. Reproductive justice (RJ) community-based organisation (CBO) SisterLove led a study on Black and Latinx women's MA perceptions and experiences in Georgia. From April 2019 to December 2020, we conducted key informant interviews with 20 abortion providers and CBO leaders and 32 in-depth interviews and 6 focus groups (<i>n</i> = 30) with Black and Latinx women. We analysed data thematically using a team-based, iterative approach of coding, memo-ing, and discussion. Participants described multilevel barriers to and strategies for MA access, wishing that \"<i>the process had a bit more humanity</i> <i> … </i> <i>[it] should be more holistic.\"</i> Barriers included (1) sociocultural factors (intersectional oppression, intersectional stigma, and medical experimentation); (2) national and state policies; (3) clinic- and provider-related factors (lack of diverse clinic staff, long waiting times); and (4) individual-level factors (lack of knowledge and social support). Suggested solutions included (1) social media campaigns and story-sharing; (2) RJ-based policy advocacy; (3) diversifying clinic staff, offering flexible scheduling and fees, community integration of abortion, and RJ abortion funds; and (4) social support (including abortion doulas) and comprehensive sex education. Findings suggest that equitable MA access for Black and Latinx communities in the post-<i>Roe</i> era will require multi-level intervention, informed by community-led evidence production; holistic, de-medicalised, and human rights-based care models; and intersectional RJ policy advocacy.</p>","PeriodicalId":37074,"journal":{"name":"Sexual and Reproductive Health Matters","volume":"30 1","pages":"2129686"},"PeriodicalIF":2.6000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0a/32/ZRHM_30_2129686.PMC9664998.pdf","citationCount":"6","resultStr":"{\"title\":\"\\\"<i>I don't regret it at all. It's just I wish the process had a bit more humanity to it … a bit more holistic</i>\\\": a qualitative, community-led medication abortion study with Black and Latinx Women in Georgia, USA.\",\"authors\":\"Elizabeth A Mosley, Sequoia Ayala, Zainab Jah, Tiffany Hailstorks, Indya Hairston, Whitney S Rice, Natalie Hernandez, Kwajelyn Jackson, Marieh Scales, Mariana Gutierrez, Bria Goode, Sofia Filippa, Shani Strader, Mariana Umbria, Autumn Watson, Joya Faruque, Adeola Raji, Janae Dunkley, Peyton Rogers, Celeste Ellison, Kheyanna Suarez, Dázon Dixon Diallo, Kelli S Hall\",\"doi\":\"10.1080/26410397.2022.2129686\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Traditional family planning research has excluded Black and Latinx leaders, and little is known about medication abortion (MA) among racial/ethnic minorities, although it is an increasingly vital reproductive health service, particularly after the fall of <i>Roe v. Wade</i>. Reproductive justice (RJ) community-based organisation (CBO) SisterLove led a study on Black and Latinx women's MA perceptions and experiences in Georgia. From April 2019 to December 2020, we conducted key informant interviews with 20 abortion providers and CBO leaders and 32 in-depth interviews and 6 focus groups (<i>n</i> = 30) with Black and Latinx women. We analysed data thematically using a team-based, iterative approach of coding, memo-ing, and discussion. Participants described multilevel barriers to and strategies for MA access, wishing that \\\"<i>the process had a bit more humanity</i> <i> … </i> <i>[it] should be more holistic.\\\"</i> Barriers included (1) sociocultural factors (intersectional oppression, intersectional stigma, and medical experimentation); (2) national and state policies; (3) clinic- and provider-related factors (lack of diverse clinic staff, long waiting times); and (4) individual-level factors (lack of knowledge and social support). Suggested solutions included (1) social media campaigns and story-sharing; (2) RJ-based policy advocacy; (3) diversifying clinic staff, offering flexible scheduling and fees, community integration of abortion, and RJ abortion funds; and (4) social support (including abortion doulas) and comprehensive sex education. Findings suggest that equitable MA access for Black and Latinx communities in the post-<i>Roe</i> era will require multi-level intervention, informed by community-led evidence production; holistic, de-medicalised, and human rights-based care models; and intersectional RJ policy advocacy.</p>\",\"PeriodicalId\":37074,\"journal\":{\"name\":\"Sexual and Reproductive Health Matters\",\"volume\":\"30 1\",\"pages\":\"2129686\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0a/32/ZRHM_30_2129686.PMC9664998.pdf\",\"citationCount\":\"6\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Sexual and Reproductive Health Matters\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1080/26410397.2022.2129686\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Sexual and Reproductive Health Matters","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1080/26410397.2022.2129686","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 6
摘要
传统的计划生育研究将黑人和拉丁裔领导人排除在外,尽管药物流产(MA)是一项日益重要的生殖健康服务,特别是在罗伊诉韦德案(Roe v. Wade)败诉之后,但人们对少数种族/族裔的药物流产(MA)知之甚少。生殖正义(RJ)社区组织(CBO) SisterLove领导了一项关于格鲁吉亚黑人和拉丁裔妇女对男性的看法和经验的研究。从2019年4月至2020年12月,我们对20名堕胎服务提供者和CBO领导人进行了关键信息访谈,并对黑人和拉丁裔妇女进行了32次深度访谈和6个焦点小组(n = 30)。我们使用基于团队的、迭代的编码、备忘录和讨论方法对数据进行了主题分析。与会者描述了MA访问的多层次障碍和策略,希望“这个过程更人性化一些……[它]应该更全面一些。”障碍包括:(1)社会文化因素(交叉压迫、交叉污名和医学实验);(2)国家政策;(3)与诊所和提供者相关的因素(缺乏多样化的诊所工作人员,等待时间长);(4)个体层面因素(缺乏知识和社会支持)。建议的解决方案包括:(1)社交媒体活动和故事分享;(2)基于责任的政策倡导;(3)多样化门诊人员,提供灵活的时间安排和收费,社区整合堕胎,RJ堕胎基金;(4)社会支持(包括人工流产助产师)和综合性教育。研究结果表明,在后罗伊案时代,黑人和拉丁裔社区公平获得医疗服务将需要多层次的干预,并以社区为主导的证据生产为依据;整体、非医疗化和基于人权的护理模式;以及交叉的RJ政策倡导。
"I don't regret it at all. It's just I wish the process had a bit more humanity to it … a bit more holistic": a qualitative, community-led medication abortion study with Black and Latinx Women in Georgia, USA.
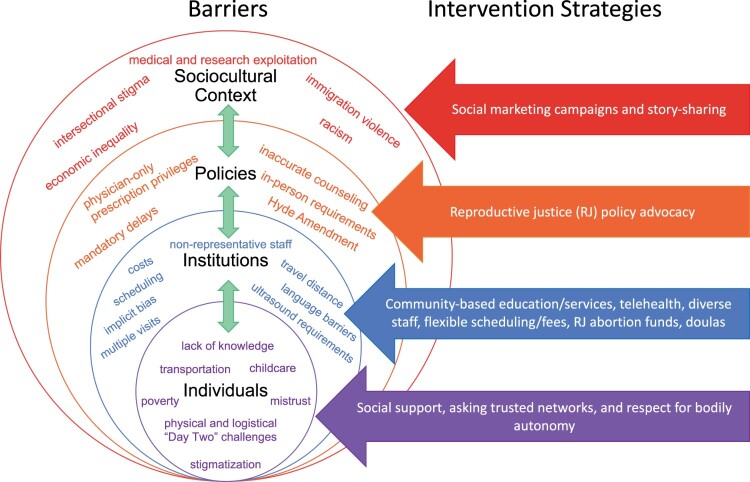
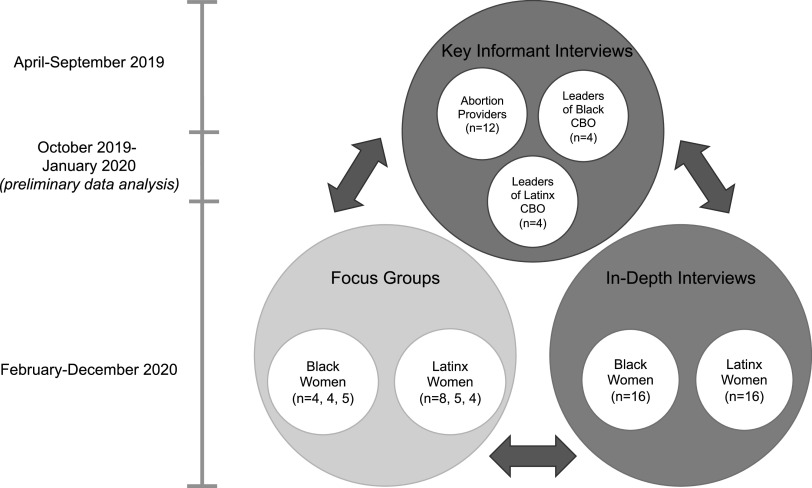
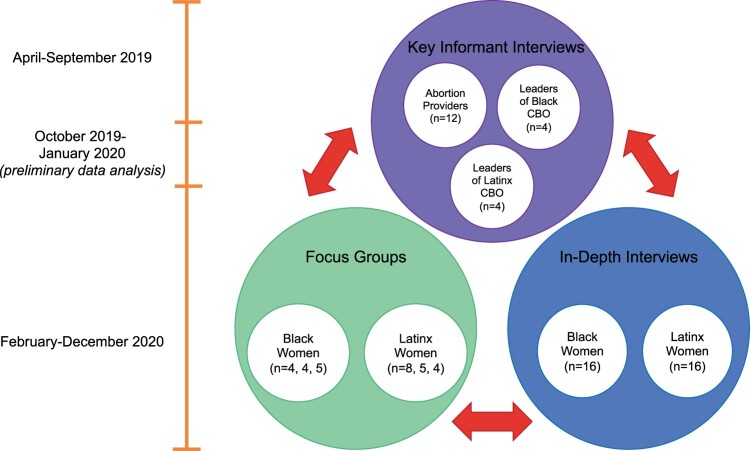
Traditional family planning research has excluded Black and Latinx leaders, and little is known about medication abortion (MA) among racial/ethnic minorities, although it is an increasingly vital reproductive health service, particularly after the fall of Roe v. Wade. Reproductive justice (RJ) community-based organisation (CBO) SisterLove led a study on Black and Latinx women's MA perceptions and experiences in Georgia. From April 2019 to December 2020, we conducted key informant interviews with 20 abortion providers and CBO leaders and 32 in-depth interviews and 6 focus groups (n = 30) with Black and Latinx women. We analysed data thematically using a team-based, iterative approach of coding, memo-ing, and discussion. Participants described multilevel barriers to and strategies for MA access, wishing that "the process had a bit more humanity … [it] should be more holistic." Barriers included (1) sociocultural factors (intersectional oppression, intersectional stigma, and medical experimentation); (2) national and state policies; (3) clinic- and provider-related factors (lack of diverse clinic staff, long waiting times); and (4) individual-level factors (lack of knowledge and social support). Suggested solutions included (1) social media campaigns and story-sharing; (2) RJ-based policy advocacy; (3) diversifying clinic staff, offering flexible scheduling and fees, community integration of abortion, and RJ abortion funds; and (4) social support (including abortion doulas) and comprehensive sex education. Findings suggest that equitable MA access for Black and Latinx communities in the post-Roe era will require multi-level intervention, informed by community-led evidence production; holistic, de-medicalised, and human rights-based care models; and intersectional RJ policy advocacy.
期刊介绍:
SRHM is a multidisciplinary journal, welcoming submissions from a wide range of disciplines, including the social sciences and humanities, behavioural science, public health, human rights and law. The journal welcomes a range of methodological approaches, including qualitative and quantitative analyses such as policy analysis; mixed methods approaches to public health and health systems research; economic, political and historical analysis; and epidemiological work with a focus on SRHR. Key topics addressed in SRHM include (but are not limited to) abortion, family planning, contraception, female genital mutilation, HIV and other STIs, human papillomavirus (HPV), maternal health, SRHR in humanitarian settings, gender-based and other forms of interpersonal violence, young people, gender, sexuality, sexual rights and sexual pleasure.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
