Roberta Cutruzzulà, Selene Laudicina, Alfredo Bagalà, Leonardo Caroti, Marilù Bartiromo, Iacopo Gianassi, Luciano Moscarelli, Lorenzo Di Maria, Aida Larti, Marco Allinovi, Giulia Antognoli, Calogero L Cirami
{"title":"肾移植后新生塌陷肾小球病:两例报告。","authors":"Roberta Cutruzzulà, Selene Laudicina, Alfredo Bagalà, Leonardo Caroti, Marilù Bartiromo, Iacopo Gianassi, Luciano Moscarelli, Lorenzo Di Maria, Aida Larti, Marco Allinovi, Giulia Antognoli, Calogero L Cirami","doi":"10.5414/CNCS110887","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Among different forms of de novo focal segmental glomerulosclerosis (FSGS), which can develop after kidney transplantation (KTx), collapsing glomerulopathy (CG) is the least frequent variant, but it is associated with the most severe form of nephrotic syndrome, histological findings of important vascular damage, and a 50% risk of graft loss. Here, we report two cases of de novo post-transplant CG.</p><p><strong>Clinical presentation: </strong>A 64-year-old White man developed proteinuria and worsening of renal function 5 years after KTx. Before the KTx, the patient was affected by an uncontrolled resistant hypertension, despite multiple antihypertensive therapies. Blood levels of calcineurin inhibitors (CNIs) were stable, with intermittent peaks. Kidney biopsy showed the presence of CG. After introduction of angiotensin receptor blockers (ARBs), urinary protein excretion progressively decreased in 6 months, but subsequent follow-up confirmed a progressive renal function decline. A 61-year-old White man developed CG 22 years after KTx. In his medical history, he was hospitalized twice to manage uncontrolled hypertensive crises. In the past, basal serum cyclosporin A levels were often detected above the therapeutic range. Low doses of intravenous methylprednisolone were administered due to the histological inflammatory signs shown on renal biopsy, followed by a rituximab infusion as a rescue therapy, but no clinical improvement was seen.</p><p><strong>Discussion and conclusion: </strong>These two cases of de novo post-transplant CG were supposed to be mainly caused by the synergic effect of metabolic factors and CNI nephrotoxicity. Identifying the etiological factors potentially responsible for de novo CG development is essential for an early therapeutic intervention and the hope of better graft and overall survival.</p>","PeriodicalId":10398,"journal":{"name":"Clinical Nephrology. Case Studies","volume":"11 ","pages":"66-71"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10127260/pdf/","citationCount":"0","resultStr":"{\"title\":\"De novo collapsing glomerulopathy after kidney transplantation: Description of two cases.\",\"authors\":\"Roberta Cutruzzulà, Selene Laudicina, Alfredo Bagalà, Leonardo Caroti, Marilù Bartiromo, Iacopo Gianassi, Luciano Moscarelli, Lorenzo Di Maria, Aida Larti, Marco Allinovi, Giulia Antognoli, Calogero L Cirami\",\"doi\":\"10.5414/CNCS110887\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Among different forms of de novo focal segmental glomerulosclerosis (FSGS), which can develop after kidney transplantation (KTx), collapsing glomerulopathy (CG) is the least frequent variant, but it is associated with the most severe form of nephrotic syndrome, histological findings of important vascular damage, and a 50% risk of graft loss. Here, we report two cases of de novo post-transplant CG.</p><p><strong>Clinical presentation: </strong>A 64-year-old White man developed proteinuria and worsening of renal function 5 years after KTx. Before the KTx, the patient was affected by an uncontrolled resistant hypertension, despite multiple antihypertensive therapies. Blood levels of calcineurin inhibitors (CNIs) were stable, with intermittent peaks. Kidney biopsy showed the presence of CG. After introduction of angiotensin receptor blockers (ARBs), urinary protein excretion progressively decreased in 6 months, but subsequent follow-up confirmed a progressive renal function decline. A 61-year-old White man developed CG 22 years after KTx. In his medical history, he was hospitalized twice to manage uncontrolled hypertensive crises. In the past, basal serum cyclosporin A levels were often detected above the therapeutic range. Low doses of intravenous methylprednisolone were administered due to the histological inflammatory signs shown on renal biopsy, followed by a rituximab infusion as a rescue therapy, but no clinical improvement was seen.</p><p><strong>Discussion and conclusion: </strong>These two cases of de novo post-transplant CG were supposed to be mainly caused by the synergic effect of metabolic factors and CNI nephrotoxicity. Identifying the etiological factors potentially responsible for de novo CG development is essential for an early therapeutic intervention and the hope of better graft and overall survival.</p>\",\"PeriodicalId\":10398,\"journal\":{\"name\":\"Clinical Nephrology. Case Studies\",\"volume\":\"11 \",\"pages\":\"66-71\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10127260/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Nephrology. Case Studies\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5414/CNCS110887\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Nephrology. Case Studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS110887","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
De novo collapsing glomerulopathy after kidney transplantation: Description of two cases.
Background: Among different forms of de novo focal segmental glomerulosclerosis (FSGS), which can develop after kidney transplantation (KTx), collapsing glomerulopathy (CG) is the least frequent variant, but it is associated with the most severe form of nephrotic syndrome, histological findings of important vascular damage, and a 50% risk of graft loss. Here, we report two cases of de novo post-transplant CG.
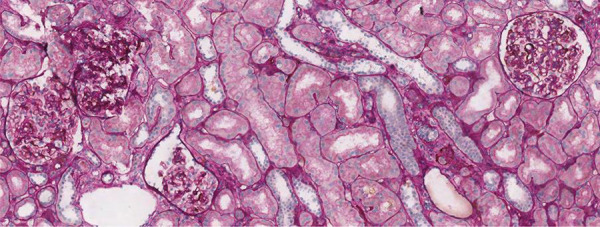
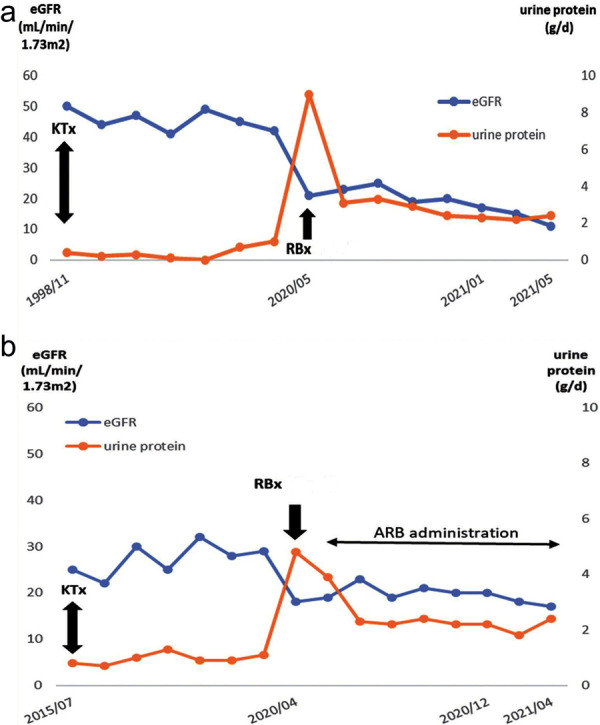
Clinical presentation: A 64-year-old White man developed proteinuria and worsening of renal function 5 years after KTx. Before the KTx, the patient was affected by an uncontrolled resistant hypertension, despite multiple antihypertensive therapies. Blood levels of calcineurin inhibitors (CNIs) were stable, with intermittent peaks. Kidney biopsy showed the presence of CG. After introduction of angiotensin receptor blockers (ARBs), urinary protein excretion progressively decreased in 6 months, but subsequent follow-up confirmed a progressive renal function decline. A 61-year-old White man developed CG 22 years after KTx. In his medical history, he was hospitalized twice to manage uncontrolled hypertensive crises. In the past, basal serum cyclosporin A levels were often detected above the therapeutic range. Low doses of intravenous methylprednisolone were administered due to the histological inflammatory signs shown on renal biopsy, followed by a rituximab infusion as a rescue therapy, but no clinical improvement was seen.
Discussion and conclusion: These two cases of de novo post-transplant CG were supposed to be mainly caused by the synergic effect of metabolic factors and CNI nephrotoxicity. Identifying the etiological factors potentially responsible for de novo CG development is essential for an early therapeutic intervention and the hope of better graft and overall survival.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
