Anna Witkowska, Tomasz Urbanowicz, Anna Olasińska-Wiśniewska, Sławomir Katarzyński, Bartłomiej Perek, Marek Jemielity
{"title":"大的无症状的梗死后左心室假性动脉瘤-在复发的冠状动脉事件中偶然发现。","authors":"Anna Witkowska, Tomasz Urbanowicz, Anna Olasińska-Wiśniewska, Sławomir Katarzyński, Bartłomiej Perek, Marek Jemielity","doi":"10.5114/kitp.2023.126099","DOIUrl":null,"url":null,"abstract":"Address for correspondence: Anna Witkowska, Department of Cardiac Surgery and Transplantology, Poznan University of Medical Sciences, Poznan, Poland, e-mail: anna.witkowska2@skpp.edu.pl Received: 14.10.2022, accepted: 5.03.2023. Left ventricular (LV) pseudoaneurysms following confined cardiac wall rupture are among mechanical complications of an acute myocardial infarction (MI), particularly if the latter one remained untreated [1]. Currently in the developed countries, early diagnosis of acute coronary syndrome (ACS) combined with reperfusion/revascularization therapies has led to the marked drop in prevalence of this complication [2]. Thus, they are considered as the rare adverse events following MI. Of note, their diagnosis might be difficult, relying mostly on the echocardiography and magnetic resonance imaging (MRI) [3]. However, it is crucial for outcomes of these patients since false aneurysms (FA) have been prone to fatal rupture. Development of LVFA can lead to heart failure, ventricular arrhythmias and thrombolytic events [4]. We present the case of a patient with a large LV pseudoaneurysm that was disclosed incidentally during hospitalization for recurrent acute coronary syndrome. A 69-year-old male, with no previous medical history, presented with an acute chest pain. He was a heavy smoker, but with no other risk factors for the coronary artery disease (CAD). On admission, the electrocardiogram (ECG) demonstrated sinus rhythm with the right bundle branch block (RBBB) and Q wave in inferior leads (II, III, AVF). The blood pressure was 115/80 mm Hg with the heart rate of 90 beats per minute and the oxygen saturation (SpO2) of 95%. Due to presence of clinical symptoms suggesting ACS combined with high serum troponin levels, the urgent coronary angiography was performed. Three-vessel disease with the subtotal stenosis of the left anterior descending artery (LAD) and circumflex artery (Cx) with total occlusion of the right coronary artery (RCA) was diagnosed. The transthoracic echocardiography revealed the LV aneurysm with maximum dimensions of 49 × 57 mm and an area of a mural thrombus (Figure 1 A), suggesting that it may be a pseudoaneurysm, LV ejection fraction (LVEF) was significantly reduced (approximately 30%). Both LV and left atrium (LA) were enlarged (73 mm and 56 mm, respectively). Additionally, moderate mitral and mild tricuspid regurgitations were observed. The cardiac MRI confirmed the echocardiographic findings in terms of both diagnosis and dimensions (42 × 73 mm). Moreover, there was an area of the mural thrombus up to 35 mm (Figure 1 B). The patient was referred for an urgent surgery and admitted to the Department of Cardiac Surgery and Transplantology for combined aneurysmectomy and coronary artery bypass grafting (CABG). A standard median sternotomy was performed. After the left internal mammary artery (LIMA) was harvested, the patient was connected to cardiopulmonary bypass (CPB) (Figure 2). With the heart arrested, the inferior wall of the LV was incised and the pseudoaneurysm was resected followed by massive clot evacuation. The edges of the ventricular wall were oversewn using two patches and 2.0 nonabsorbable monofilament suture. The LAD was grafted with LIMA. There was no possibility for RCA grafting due to the pseudoaneurysm location and small diameter of the artery. The patient was successfully weaned from cardiopulmonary bypass (CPB) and after chest closure was transferred to the intensive care unit. The patient had uneventful recovery and was discharged home on the 7th day after surgery. Post-operative echocardiography showed markedly improved LVEF (about 50%) and only mild mitral regurgitation. Diameters of the LV decreased to 52 mm and that of the LA to 35 mm. According to the ESC (European Society of Cardiology)/ EACTS (European Association for Cardio-Thoracic Surgery) guidelines on myocardial revascularization [5], LV aneurysmectomy during CABG should be considered in patients with NYHA class III/IV, large LV aneurysm, large thrombus formation, or if the aneurysm is the origin of arrhythmias. We are convinced that our patient, although relatively asymptomatic regarding LV aneurysm itself, had clear indications to have the aneurysm excised due to its dimension and thrombus inside. Additionally, good early outcomes confirmed the appropriate decision to qualify the patient for urgent surgery and A large asymptomatic postinfarction left ventricular pseudoaneurysm – an incidental finding during a recurrent coronary event","PeriodicalId":49945,"journal":{"name":"Kardiochirurgia I Torakochirurgia Polska","volume":"20 1","pages":"47-49"},"PeriodicalIF":1.3000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b6/96/KITP-20-50412.PMC10107411.pdf","citationCount":"0","resultStr":"{\"title\":\"A large asymptomatic postinfarction left ventricular pseudoaneurysm - an incidental finding during a recurrent coronary event.\",\"authors\":\"Anna Witkowska, Tomasz Urbanowicz, Anna Olasińska-Wiśniewska, Sławomir Katarzyński, Bartłomiej Perek, Marek Jemielity\",\"doi\":\"10.5114/kitp.2023.126099\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Address for correspondence: Anna Witkowska, Department of Cardiac Surgery and Transplantology, Poznan University of Medical Sciences, Poznan, Poland, e-mail: anna.witkowska2@skpp.edu.pl Received: 14.10.2022, accepted: 5.03.2023. Left ventricular (LV) pseudoaneurysms following confined cardiac wall rupture are among mechanical complications of an acute myocardial infarction (MI), particularly if the latter one remained untreated [1]. Currently in the developed countries, early diagnosis of acute coronary syndrome (ACS) combined with reperfusion/revascularization therapies has led to the marked drop in prevalence of this complication [2]. Thus, they are considered as the rare adverse events following MI. Of note, their diagnosis might be difficult, relying mostly on the echocardiography and magnetic resonance imaging (MRI) [3]. However, it is crucial for outcomes of these patients since false aneurysms (FA) have been prone to fatal rupture. Development of LVFA can lead to heart failure, ventricular arrhythmias and thrombolytic events [4]. We present the case of a patient with a large LV pseudoaneurysm that was disclosed incidentally during hospitalization for recurrent acute coronary syndrome. A 69-year-old male, with no previous medical history, presented with an acute chest pain. He was a heavy smoker, but with no other risk factors for the coronary artery disease (CAD). On admission, the electrocardiogram (ECG) demonstrated sinus rhythm with the right bundle branch block (RBBB) and Q wave in inferior leads (II, III, AVF). The blood pressure was 115/80 mm Hg with the heart rate of 90 beats per minute and the oxygen saturation (SpO2) of 95%. Due to presence of clinical symptoms suggesting ACS combined with high serum troponin levels, the urgent coronary angiography was performed. Three-vessel disease with the subtotal stenosis of the left anterior descending artery (LAD) and circumflex artery (Cx) with total occlusion of the right coronary artery (RCA) was diagnosed. The transthoracic echocardiography revealed the LV aneurysm with maximum dimensions of 49 × 57 mm and an area of a mural thrombus (Figure 1 A), suggesting that it may be a pseudoaneurysm, LV ejection fraction (LVEF) was significantly reduced (approximately 30%). Both LV and left atrium (LA) were enlarged (73 mm and 56 mm, respectively). Additionally, moderate mitral and mild tricuspid regurgitations were observed. The cardiac MRI confirmed the echocardiographic findings in terms of both diagnosis and dimensions (42 × 73 mm). Moreover, there was an area of the mural thrombus up to 35 mm (Figure 1 B). The patient was referred for an urgent surgery and admitted to the Department of Cardiac Surgery and Transplantology for combined aneurysmectomy and coronary artery bypass grafting (CABG). A standard median sternotomy was performed. After the left internal mammary artery (LIMA) was harvested, the patient was connected to cardiopulmonary bypass (CPB) (Figure 2). With the heart arrested, the inferior wall of the LV was incised and the pseudoaneurysm was resected followed by massive clot evacuation. The edges of the ventricular wall were oversewn using two patches and 2.0 nonabsorbable monofilament suture. The LAD was grafted with LIMA. There was no possibility for RCA grafting due to the pseudoaneurysm location and small diameter of the artery. The patient was successfully weaned from cardiopulmonary bypass (CPB) and after chest closure was transferred to the intensive care unit. The patient had uneventful recovery and was discharged home on the 7th day after surgery. Post-operative echocardiography showed markedly improved LVEF (about 50%) and only mild mitral regurgitation. Diameters of the LV decreased to 52 mm and that of the LA to 35 mm. According to the ESC (European Society of Cardiology)/ EACTS (European Association for Cardio-Thoracic Surgery) guidelines on myocardial revascularization [5], LV aneurysmectomy during CABG should be considered in patients with NYHA class III/IV, large LV aneurysm, large thrombus formation, or if the aneurysm is the origin of arrhythmias. We are convinced that our patient, although relatively asymptomatic regarding LV aneurysm itself, had clear indications to have the aneurysm excised due to its dimension and thrombus inside. Additionally, good early outcomes confirmed the appropriate decision to qualify the patient for urgent surgery and A large asymptomatic postinfarction left ventricular pseudoaneurysm – an incidental finding during a recurrent coronary event\",\"PeriodicalId\":49945,\"journal\":{\"name\":\"Kardiochirurgia I Torakochirurgia Polska\",\"volume\":\"20 1\",\"pages\":\"47-49\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2023-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b6/96/KITP-20-50412.PMC10107411.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Kardiochirurgia I Torakochirurgia Polska\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5114/kitp.2023.126099\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Kardiochirurgia I Torakochirurgia Polska","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/kitp.2023.126099","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
A large asymptomatic postinfarction left ventricular pseudoaneurysm - an incidental finding during a recurrent coronary event.
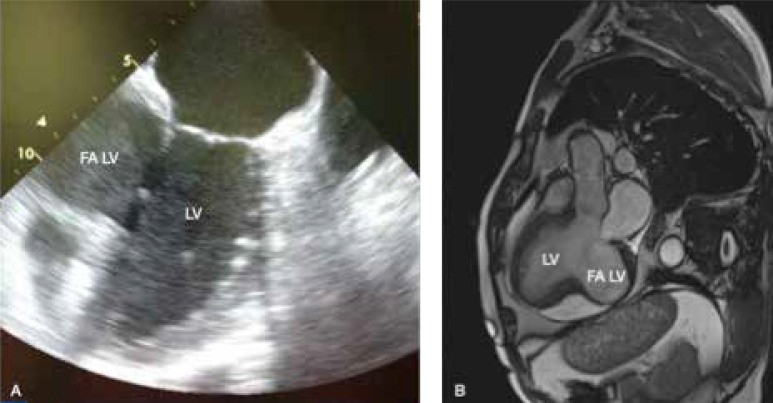
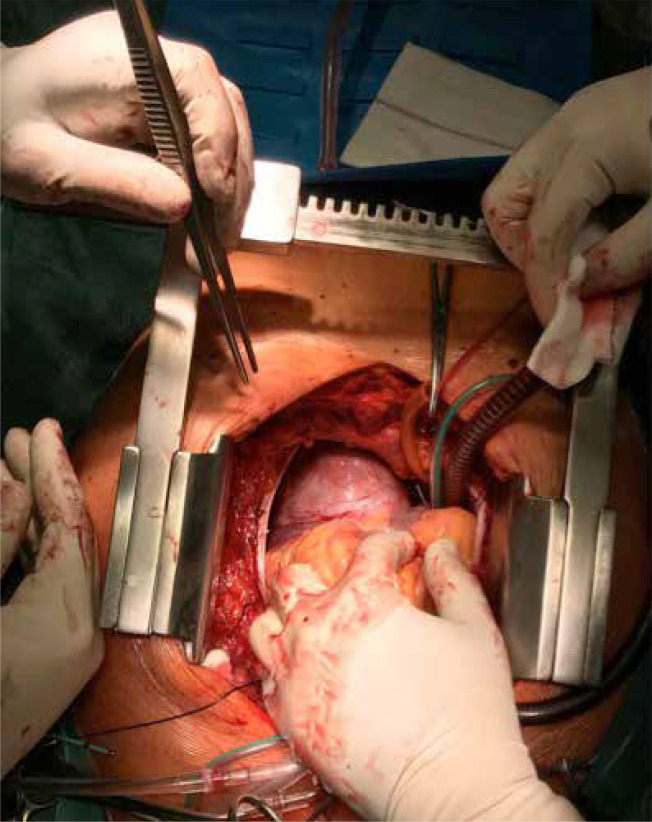
Address for correspondence: Anna Witkowska, Department of Cardiac Surgery and Transplantology, Poznan University of Medical Sciences, Poznan, Poland, e-mail: anna.witkowska2@skpp.edu.pl Received: 14.10.2022, accepted: 5.03.2023. Left ventricular (LV) pseudoaneurysms following confined cardiac wall rupture are among mechanical complications of an acute myocardial infarction (MI), particularly if the latter one remained untreated [1]. Currently in the developed countries, early diagnosis of acute coronary syndrome (ACS) combined with reperfusion/revascularization therapies has led to the marked drop in prevalence of this complication [2]. Thus, they are considered as the rare adverse events following MI. Of note, their diagnosis might be difficult, relying mostly on the echocardiography and magnetic resonance imaging (MRI) [3]. However, it is crucial for outcomes of these patients since false aneurysms (FA) have been prone to fatal rupture. Development of LVFA can lead to heart failure, ventricular arrhythmias and thrombolytic events [4]. We present the case of a patient with a large LV pseudoaneurysm that was disclosed incidentally during hospitalization for recurrent acute coronary syndrome. A 69-year-old male, with no previous medical history, presented with an acute chest pain. He was a heavy smoker, but with no other risk factors for the coronary artery disease (CAD). On admission, the electrocardiogram (ECG) demonstrated sinus rhythm with the right bundle branch block (RBBB) and Q wave in inferior leads (II, III, AVF). The blood pressure was 115/80 mm Hg with the heart rate of 90 beats per minute and the oxygen saturation (SpO2) of 95%. Due to presence of clinical symptoms suggesting ACS combined with high serum troponin levels, the urgent coronary angiography was performed. Three-vessel disease with the subtotal stenosis of the left anterior descending artery (LAD) and circumflex artery (Cx) with total occlusion of the right coronary artery (RCA) was diagnosed. The transthoracic echocardiography revealed the LV aneurysm with maximum dimensions of 49 × 57 mm and an area of a mural thrombus (Figure 1 A), suggesting that it may be a pseudoaneurysm, LV ejection fraction (LVEF) was significantly reduced (approximately 30%). Both LV and left atrium (LA) were enlarged (73 mm and 56 mm, respectively). Additionally, moderate mitral and mild tricuspid regurgitations were observed. The cardiac MRI confirmed the echocardiographic findings in terms of both diagnosis and dimensions (42 × 73 mm). Moreover, there was an area of the mural thrombus up to 35 mm (Figure 1 B). The patient was referred for an urgent surgery and admitted to the Department of Cardiac Surgery and Transplantology for combined aneurysmectomy and coronary artery bypass grafting (CABG). A standard median sternotomy was performed. After the left internal mammary artery (LIMA) was harvested, the patient was connected to cardiopulmonary bypass (CPB) (Figure 2). With the heart arrested, the inferior wall of the LV was incised and the pseudoaneurysm was resected followed by massive clot evacuation. The edges of the ventricular wall were oversewn using two patches and 2.0 nonabsorbable monofilament suture. The LAD was grafted with LIMA. There was no possibility for RCA grafting due to the pseudoaneurysm location and small diameter of the artery. The patient was successfully weaned from cardiopulmonary bypass (CPB) and after chest closure was transferred to the intensive care unit. The patient had uneventful recovery and was discharged home on the 7th day after surgery. Post-operative echocardiography showed markedly improved LVEF (about 50%) and only mild mitral regurgitation. Diameters of the LV decreased to 52 mm and that of the LA to 35 mm. According to the ESC (European Society of Cardiology)/ EACTS (European Association for Cardio-Thoracic Surgery) guidelines on myocardial revascularization [5], LV aneurysmectomy during CABG should be considered in patients with NYHA class III/IV, large LV aneurysm, large thrombus formation, or if the aneurysm is the origin of arrhythmias. We are convinced that our patient, although relatively asymptomatic regarding LV aneurysm itself, had clear indications to have the aneurysm excised due to its dimension and thrombus inside. Additionally, good early outcomes confirmed the appropriate decision to qualify the patient for urgent surgery and A large asymptomatic postinfarction left ventricular pseudoaneurysm – an incidental finding during a recurrent coronary event
期刊介绍:
Polish Journal of Thoracic and Cardiovascular Surgery is a quarterly aimed at cardiologists, cardiosurgeons and thoracic surgeons. Includes the original works (experimental, research and development), illustrative and casuistical works about cardiology and cardiosurgery.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
