{"title":"[桡骨远端畸形:关节内和关节外矫正截骨的3D规划和性能]。","authors":"Raffael Labèr, Andreas Schweizer","doi":"10.1007/s00064-023-00808-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Restoration of the original anatomy with reduction of both current symptoms and risk of posttraumatic osteoarthritis.</p><p><strong>Indications: </strong>Symptomatic intra- or extra-articular malunion due to limitation of movement and/or painful function, intra-articular step of > 1 mm, instability of the distal radioulnar joint.</p><p><strong>Contraindications: </strong>Minimal deformity. Pre-existing osteoarthritis Knirk and Jupiter II or higher. Simpler surgical alternative, e.g., ulna shortening osteotomy. Smoking or advanced age are not contraindications.</p><p><strong>Surgical technique: </strong>Preoperative assessment and performance of a bilateral computed tomography (CT). Three-dimensional (3D) malposition analysis and calculation of the correction. Planning of the corrective osteotomy on the 3D model and creation of patient-specific drilling and sawing guides. Performing the 3D-guided osteotomy.</p><p><strong>Postoperative management: </strong>Early functional unloaded mobilization with the splint for 8 weeks until consolidation control with CT.</p><p><strong>Results: </strong>Significant reduction of the step to < 1 mm (p ≤ 0.05) can be achieved with intra-articular corrections. In extra-articular corrective osteotomies, a mean residual rotational malalignment error of 2.0° (± 2.2°) and a translational malalignment error of 0.6 mm (± 0.2 mm) is achieved. Single-cut osteotomies in the shaft region can be performed to within a few degrees for rotation (e.g., pronation/supination 4.9°) and for translation (e.g., proximal/distal, 0.8 mm). After surgery, a mean residual 3D angle of 5.8° (SD 3.6°) was measured. Furthermore, surgical time for 3D-assisted surgery is significantly reduced compared to the conventional technique (140 ± 37 vs 108 ± 26 min; p < 0.05). Thus, the progression of osteoarthritis can be reduced in the medium term and improved mobility and grip strength are achieved. The clinical outcome parameters based on patient-rated wrist evaluation (PRWE) and the disabilities of the arm, shoulder and hand (DASH) scores are roughly comparable.</p>","PeriodicalId":54677,"journal":{"name":"Operative Orthopadie Und Traumatologie","volume":" ","pages":"258-269"},"PeriodicalIF":1.0000,"publicationDate":"2023-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10520186/pdf/","citationCount":"0","resultStr":"{\"title\":\"[Malunion of the distal radius: 3D planning and performance of intra- and extra-articular corrective osteotomy].\",\"authors\":\"Raffael Labèr, Andreas Schweizer\",\"doi\":\"10.1007/s00064-023-00808-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Restoration of the original anatomy with reduction of both current symptoms and risk of posttraumatic osteoarthritis.</p><p><strong>Indications: </strong>Symptomatic intra- or extra-articular malunion due to limitation of movement and/or painful function, intra-articular step of > 1 mm, instability of the distal radioulnar joint.</p><p><strong>Contraindications: </strong>Minimal deformity. Pre-existing osteoarthritis Knirk and Jupiter II or higher. Simpler surgical alternative, e.g., ulna shortening osteotomy. Smoking or advanced age are not contraindications.</p><p><strong>Surgical technique: </strong>Preoperative assessment and performance of a bilateral computed tomography (CT). Three-dimensional (3D) malposition analysis and calculation of the correction. Planning of the corrective osteotomy on the 3D model and creation of patient-specific drilling and sawing guides. Performing the 3D-guided osteotomy.</p><p><strong>Postoperative management: </strong>Early functional unloaded mobilization with the splint for 8 weeks until consolidation control with CT.</p><p><strong>Results: </strong>Significant reduction of the step to < 1 mm (p ≤ 0.05) can be achieved with intra-articular corrections. In extra-articular corrective osteotomies, a mean residual rotational malalignment error of 2.0° (± 2.2°) and a translational malalignment error of 0.6 mm (± 0.2 mm) is achieved. Single-cut osteotomies in the shaft region can be performed to within a few degrees for rotation (e.g., pronation/supination 4.9°) and for translation (e.g., proximal/distal, 0.8 mm). After surgery, a mean residual 3D angle of 5.8° (SD 3.6°) was measured. Furthermore, surgical time for 3D-assisted surgery is significantly reduced compared to the conventional technique (140 ± 37 vs 108 ± 26 min; p < 0.05). Thus, the progression of osteoarthritis can be reduced in the medium term and improved mobility and grip strength are achieved. The clinical outcome parameters based on patient-rated wrist evaluation (PRWE) and the disabilities of the arm, shoulder and hand (DASH) scores are roughly comparable.</p>\",\"PeriodicalId\":54677,\"journal\":{\"name\":\"Operative Orthopadie Und Traumatologie\",\"volume\":\" \",\"pages\":\"258-269\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2023-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10520186/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Operative Orthopadie Und Traumatologie\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00064-023-00808-8\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/5/2 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Operative Orthopadie Und Traumatologie","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00064-023-00808-8","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/5/2 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
[Malunion of the distal radius: 3D planning and performance of intra- and extra-articular corrective osteotomy].
Objective: Restoration of the original anatomy with reduction of both current symptoms and risk of posttraumatic osteoarthritis.
Indications: Symptomatic intra- or extra-articular malunion due to limitation of movement and/or painful function, intra-articular step of > 1 mm, instability of the distal radioulnar joint.
Contraindications: Minimal deformity. Pre-existing osteoarthritis Knirk and Jupiter II or higher. Simpler surgical alternative, e.g., ulna shortening osteotomy. Smoking or advanced age are not contraindications.
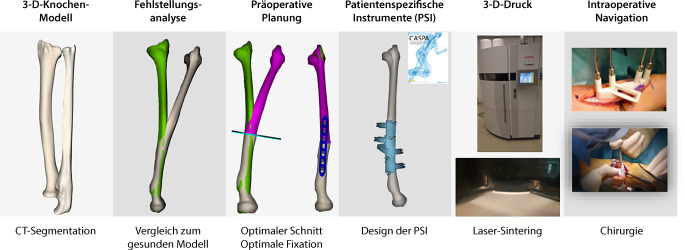
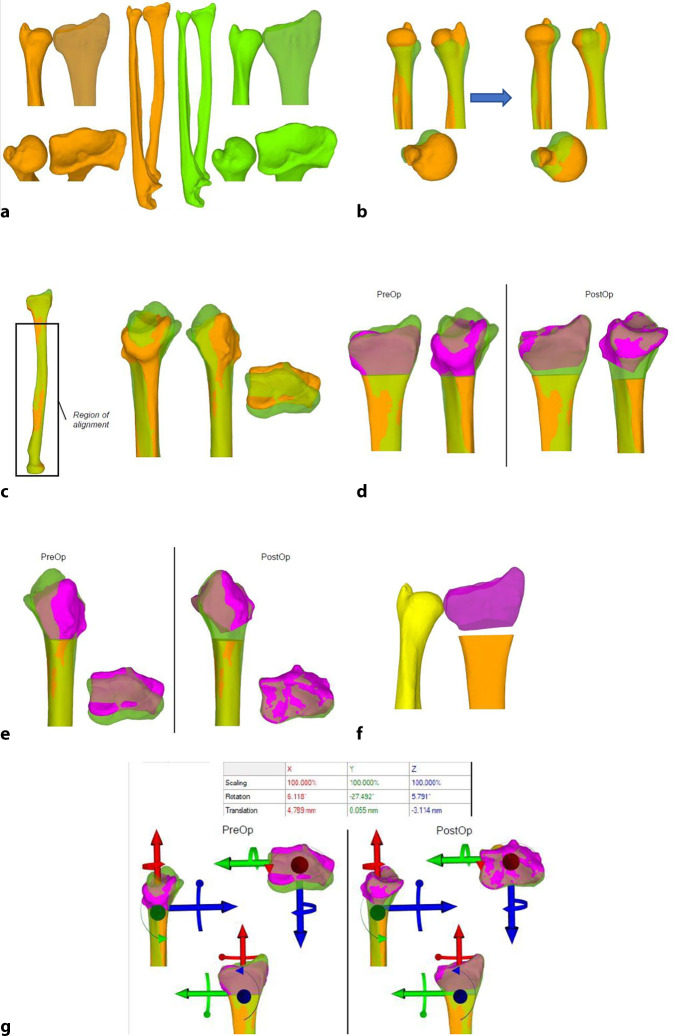
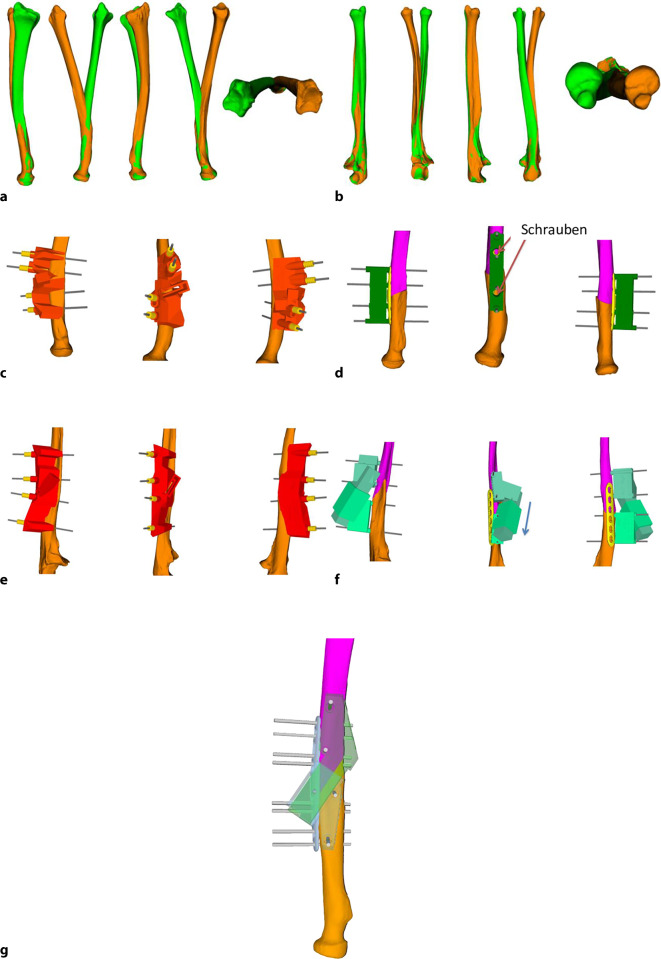
Surgical technique: Preoperative assessment and performance of a bilateral computed tomography (CT). Three-dimensional (3D) malposition analysis and calculation of the correction. Planning of the corrective osteotomy on the 3D model and creation of patient-specific drilling and sawing guides. Performing the 3D-guided osteotomy.
Postoperative management: Early functional unloaded mobilization with the splint for 8 weeks until consolidation control with CT.
Results: Significant reduction of the step to < 1 mm (p ≤ 0.05) can be achieved with intra-articular corrections. In extra-articular corrective osteotomies, a mean residual rotational malalignment error of 2.0° (± 2.2°) and a translational malalignment error of 0.6 mm (± 0.2 mm) is achieved. Single-cut osteotomies in the shaft region can be performed to within a few degrees for rotation (e.g., pronation/supination 4.9°) and for translation (e.g., proximal/distal, 0.8 mm). After surgery, a mean residual 3D angle of 5.8° (SD 3.6°) was measured. Furthermore, surgical time for 3D-assisted surgery is significantly reduced compared to the conventional technique (140 ± 37 vs 108 ± 26 min; p < 0.05). Thus, the progression of osteoarthritis can be reduced in the medium term and improved mobility and grip strength are achieved. The clinical outcome parameters based on patient-rated wrist evaluation (PRWE) and the disabilities of the arm, shoulder and hand (DASH) scores are roughly comparable.
期刊介绍:
Orthopedics and Traumatology is directed toward all orthopedic surgeons, trauma-tologists, hand surgeons, specialists in sports injuries, orthopedics and rheumatology as well as gene-al surgeons who require access to reliable information on current operative methods to ensure the quality of patient advice, preoperative planning, and postoperative care.
The journal presents established and new operative procedures in uniformly structured and extensively illustrated contributions. All aspects are presented step-by-step from indications, contraindications, patient education, and preparation of the operation right through to postoperative care. The advantages and disadvantages, possible complications, deficiencies and risks of the methods as well as significant results with their evaluation criteria are discussed. To allow the reader to assess the outcome, results are detailed and based on internationally recognized scoring systems.
Orthopedics and Traumatology facilitates effective advancement and further education for all those active in both special and conservative fields of orthopedics, traumatology, and general surgery, offers sup-port for therapeutic decision-making, and provides – more than 30 years after its first publication – constantly expanding and up-to-date teaching on operative techniques.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
