{"title":"下颌骨成釉细胞癌1例。","authors":"Satoru Ogane, Arisa Fujii, Taiki Suzuki, Kazuhiko Hashimoto, Sadamitsu Hashimoto, Masayuki Takano, Akira Katakura, Takeshi Nomura","doi":"10.1186/s40902-023-00380-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Ameloblastic carcinoma is a malignant form of ameloblastoma and a very rare odontogenic tumor. We report a case of ameloblastic carcinoma that occurred after removal of a right-sided mandibular dental implant.</p><p><strong>Case presentation: </strong>A 72-year-old female patient visited her family dentist with a complaint of pain around a lower right implant placed 37 years previously. Although the dental implant was removed with the diagnosis of peri-implantitis, the patient experienced dullness of sensation in the lower lip and was followed up by her dentist, but after no improvement. She was referred to a highly specialized institution where she was diagnosed with osteomyelitis and treated the patient with medication; however, there was no improvement. In addition, granulation was observed in the same area leading to a suspicion of malignancy, and the patient was referred to our oral cancer center. The diagnosis of squamous cell carcinoma was made after a biopsy at our hospital. Under general anesthesia, the patient underwent mandibulectomy, right-sided neck dissection, free flap reconstruction with an anterolateral thigh flap, immediate reconstruction with a metal plate, and tracheostomy. Histological analysis of the resected specimen on hematoxylin and eosin staining showed structures reminiscent of enamel pulp and squamous epithelium in the center of the tumor. The tumor cells were highly atypical, with nuclear staining, hypertrophy, irregular nuclear size, and irregular nuclear shape, all of which were suggestive of cancer. Immunohistochemical analysis showed that Ki-67 was expressed in more than 80% of the targeted area, and the final diagnosis was primary ameloblastic carcinoma.</p><p><strong>Conclusion: </strong>After reconstructive flap transplantation, occlusion was re-established using a maxillofacial prosthesis. The patient remained disease-free at the 1-year 3-month follow-up.</p>","PeriodicalId":18357,"journal":{"name":"Maxillofacial Plastic and Reconstructive Surgery","volume":"45 1","pages":"17"},"PeriodicalIF":2.8000,"publicationDate":"2023-04-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10133431/pdf/","citationCount":"0","resultStr":"{\"title\":\"Ameloblastic carcinoma of the mandible: a case report.\",\"authors\":\"Satoru Ogane, Arisa Fujii, Taiki Suzuki, Kazuhiko Hashimoto, Sadamitsu Hashimoto, Masayuki Takano, Akira Katakura, Takeshi Nomura\",\"doi\":\"10.1186/s40902-023-00380-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Ameloblastic carcinoma is a malignant form of ameloblastoma and a very rare odontogenic tumor. We report a case of ameloblastic carcinoma that occurred after removal of a right-sided mandibular dental implant.</p><p><strong>Case presentation: </strong>A 72-year-old female patient visited her family dentist with a complaint of pain around a lower right implant placed 37 years previously. Although the dental implant was removed with the diagnosis of peri-implantitis, the patient experienced dullness of sensation in the lower lip and was followed up by her dentist, but after no improvement. She was referred to a highly specialized institution where she was diagnosed with osteomyelitis and treated the patient with medication; however, there was no improvement. In addition, granulation was observed in the same area leading to a suspicion of malignancy, and the patient was referred to our oral cancer center. The diagnosis of squamous cell carcinoma was made after a biopsy at our hospital. Under general anesthesia, the patient underwent mandibulectomy, right-sided neck dissection, free flap reconstruction with an anterolateral thigh flap, immediate reconstruction with a metal plate, and tracheostomy. Histological analysis of the resected specimen on hematoxylin and eosin staining showed structures reminiscent of enamel pulp and squamous epithelium in the center of the tumor. The tumor cells were highly atypical, with nuclear staining, hypertrophy, irregular nuclear size, and irregular nuclear shape, all of which were suggestive of cancer. Immunohistochemical analysis showed that Ki-67 was expressed in more than 80% of the targeted area, and the final diagnosis was primary ameloblastic carcinoma.</p><p><strong>Conclusion: </strong>After reconstructive flap transplantation, occlusion was re-established using a maxillofacial prosthesis. The patient remained disease-free at the 1-year 3-month follow-up.</p>\",\"PeriodicalId\":18357,\"journal\":{\"name\":\"Maxillofacial Plastic and Reconstructive Surgery\",\"volume\":\"45 1\",\"pages\":\"17\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2023-04-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10133431/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Maxillofacial Plastic and Reconstructive Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40902-023-00380-y\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"DENTISTRY, ORAL SURGERY & MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Maxillofacial Plastic and Reconstructive Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40902-023-00380-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"DENTISTRY, ORAL SURGERY & MEDICINE","Score":null,"Total":0}
Ameloblastic carcinoma of the mandible: a case report.
Background: Ameloblastic carcinoma is a malignant form of ameloblastoma and a very rare odontogenic tumor. We report a case of ameloblastic carcinoma that occurred after removal of a right-sided mandibular dental implant.
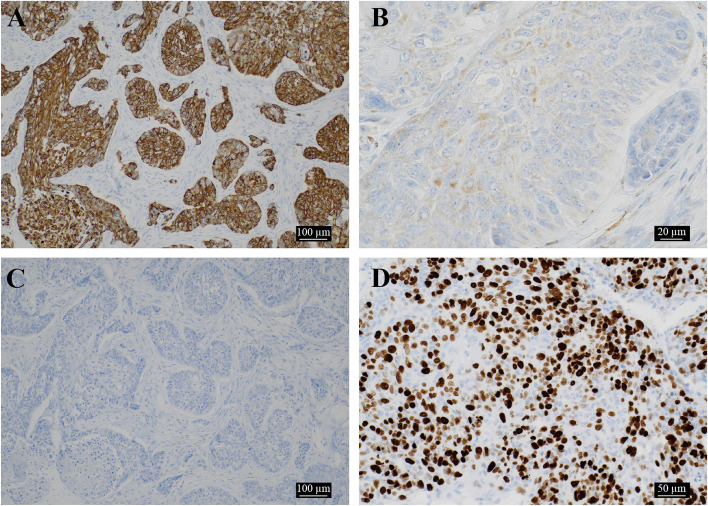
Case presentation: A 72-year-old female patient visited her family dentist with a complaint of pain around a lower right implant placed 37 years previously. Although the dental implant was removed with the diagnosis of peri-implantitis, the patient experienced dullness of sensation in the lower lip and was followed up by her dentist, but after no improvement. She was referred to a highly specialized institution where she was diagnosed with osteomyelitis and treated the patient with medication; however, there was no improvement. In addition, granulation was observed in the same area leading to a suspicion of malignancy, and the patient was referred to our oral cancer center. The diagnosis of squamous cell carcinoma was made after a biopsy at our hospital. Under general anesthesia, the patient underwent mandibulectomy, right-sided neck dissection, free flap reconstruction with an anterolateral thigh flap, immediate reconstruction with a metal plate, and tracheostomy. Histological analysis of the resected specimen on hematoxylin and eosin staining showed structures reminiscent of enamel pulp and squamous epithelium in the center of the tumor. The tumor cells were highly atypical, with nuclear staining, hypertrophy, irregular nuclear size, and irregular nuclear shape, all of which were suggestive of cancer. Immunohistochemical analysis showed that Ki-67 was expressed in more than 80% of the targeted area, and the final diagnosis was primary ameloblastic carcinoma.
Conclusion: After reconstructive flap transplantation, occlusion was re-established using a maxillofacial prosthesis. The patient remained disease-free at the 1-year 3-month follow-up.






 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
