Serge A Steenen, Roos van Westrhenen, Jan de Lange, Ad de Jongh
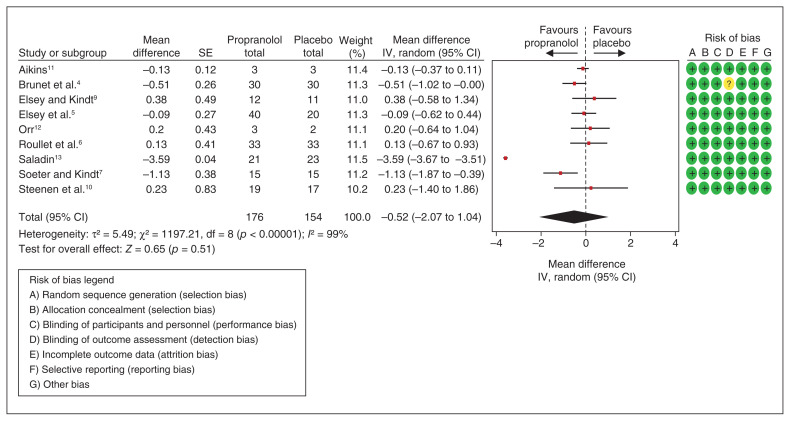
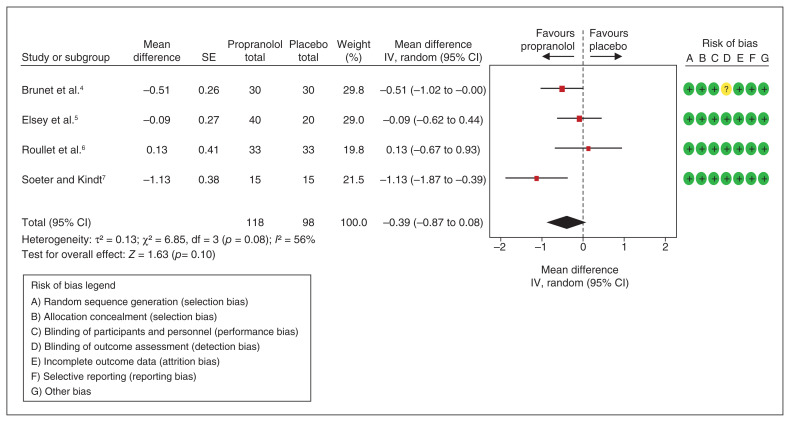
{"title":"更新和修正的荟萃分析显示,心得安与安慰剂对创伤性记忆再巩固中断没有影响。","authors":"Serge A Steenen, Roos van Westrhenen, Jan de Lange, Ad de Jongh","doi":"10.1503/jpn.220072-l","DOIUrl":null,"url":null,"abstract":"","PeriodicalId":50073,"journal":{"name":"Journal of Psychiatry & Neuroscience","volume":"47 5","pages":"E336-E337"},"PeriodicalIF":3.3000,"publicationDate":"2022-09-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b4/6e/47-5-E336.PMC9640173.pdf","citationCount":"0","resultStr":"{\"title\":\"Updated and rectified meta-analysis shows no effect of propranolol versus placebo on traumatic memory reconsolidation disruption.\",\"authors\":\"Serge A Steenen, Roos van Westrhenen, Jan de Lange, Ad de Jongh\",\"doi\":\"10.1503/jpn.220072-l\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"\",\"PeriodicalId\":50073,\"journal\":{\"name\":\"Journal of Psychiatry & Neuroscience\",\"volume\":\"47 5\",\"pages\":\"E336-E337\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2022-09-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b4/6e/47-5-E336.PMC9640173.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Psychiatry & Neuroscience\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1503/jpn.220072-l\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/9/1 0:00:00\",\"PubModel\":\"Print\",\"JCR\":\"Q2\",\"JCRName\":\"NEUROSCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Psychiatry & Neuroscience","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1503/jpn.220072-l","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/9/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"NEUROSCIENCES","Score":null,"Total":0}
期刊介绍:
The Journal of Psychiatry & Neuroscience publishes papers at the intersection of psychiatry and neuroscience that advance our understanding of the neural mechanisms involved in the etiology and treatment of psychiatric disorders. This includes studies on patients with psychiatric disorders, healthy humans, and experimental animals as well as studies in vitro. Original research articles, including clinical trials with a mechanistic component, and review papers will be considered.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
