Zibya Barday, Malcolm Masikati, Nicola Wearne, Brian Rayner, Bianca Davidson, Kathleen Jane Bateman, Erika Jones
{"title":"原发性干燥综合征伴肾小管酸中毒和脑桥中央髓鞘溶解:一种不寻常的三联征。","authors":"Zibya Barday, Malcolm Masikati, Nicola Wearne, Brian Rayner, Bianca Davidson, Kathleen Jane Bateman, Erika Jones","doi":"10.5414/CNCS110994","DOIUrl":null,"url":null,"abstract":"<p><p>Primary Sjögren's syndrome (pSS) is a complex, multisystem autoimmune disorder. It is characterized by lymphocytic infiltration of the exocrine glands. In the setting of pSS, the presence of systemic disease is an important prognostic determinant, but involvement of the kidney is uncommon. The triad of pSS, distal renal tubular acidosis (dRTA), and central pontine myelinolysis (CPM) is rare and potentially fatal. A 42-year-old woman presented with dRTA, profound hypokalemia, and CPM characterized by progressive global quadriparesis, ophthalmoplegia, and encephalopathy. Sjögren's syndrome was diagnosed based on sicca symptoms, clinical features, and strongly positive anti-SSA/Ro and anti-SSB/La autoantibodies. The patient responded well to electrolyte replacement, acid-base correction, corticosteroids, and subsequent cyclophosphamide therapy. Early recognition and appropriate treatment resulted in good kidney and neurological outcomes in this case. This report highlights the need to consider the diagnosis of pSS in unexplained dRTA and CPM, as it has a favorable prognosis if recognized and managed timeously.</p>","PeriodicalId":10398,"journal":{"name":"Clinical Nephrology. Case Studies","volume":"11 ","pages":"79-86"},"PeriodicalIF":0.0000,"publicationDate":"2023-05-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10167752/pdf/","citationCount":"1","resultStr":"{\"title\":\"Primary Sjögren's syndrome with renal tubular acidosis and central pontine myelinolysis: An unusual triad.\",\"authors\":\"Zibya Barday, Malcolm Masikati, Nicola Wearne, Brian Rayner, Bianca Davidson, Kathleen Jane Bateman, Erika Jones\",\"doi\":\"10.5414/CNCS110994\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Primary Sjögren's syndrome (pSS) is a complex, multisystem autoimmune disorder. It is characterized by lymphocytic infiltration of the exocrine glands. In the setting of pSS, the presence of systemic disease is an important prognostic determinant, but involvement of the kidney is uncommon. The triad of pSS, distal renal tubular acidosis (dRTA), and central pontine myelinolysis (CPM) is rare and potentially fatal. A 42-year-old woman presented with dRTA, profound hypokalemia, and CPM characterized by progressive global quadriparesis, ophthalmoplegia, and encephalopathy. Sjögren's syndrome was diagnosed based on sicca symptoms, clinical features, and strongly positive anti-SSA/Ro and anti-SSB/La autoantibodies. The patient responded well to electrolyte replacement, acid-base correction, corticosteroids, and subsequent cyclophosphamide therapy. Early recognition and appropriate treatment resulted in good kidney and neurological outcomes in this case. This report highlights the need to consider the diagnosis of pSS in unexplained dRTA and CPM, as it has a favorable prognosis if recognized and managed timeously.</p>\",\"PeriodicalId\":10398,\"journal\":{\"name\":\"Clinical Nephrology. Case Studies\",\"volume\":\"11 \",\"pages\":\"79-86\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-05-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10167752/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Nephrology. Case Studies\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5414/CNCS110994\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Nephrology. Case Studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS110994","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Primary Sjögren's syndrome with renal tubular acidosis and central pontine myelinolysis: An unusual triad.
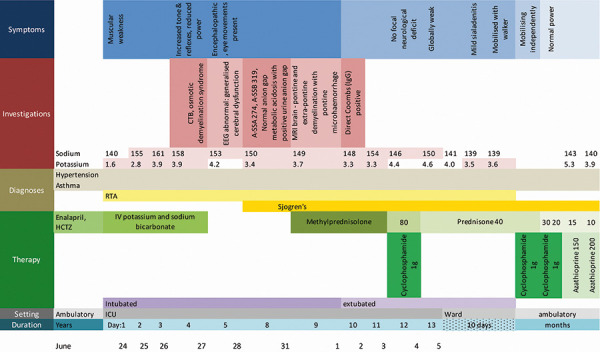
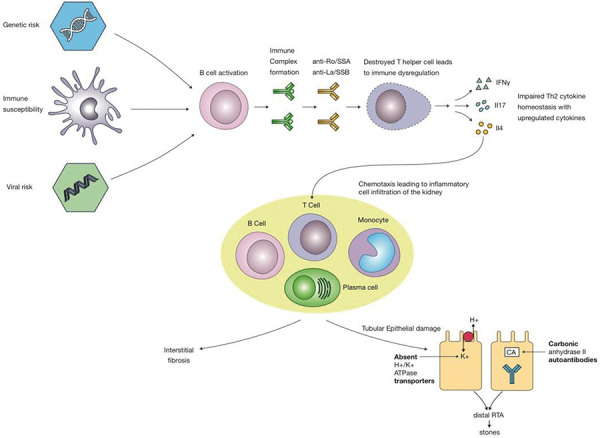
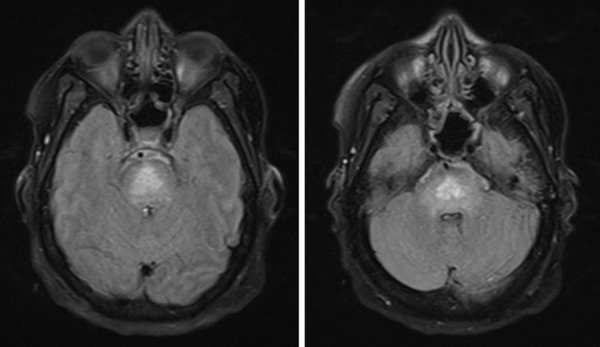
Primary Sjögren's syndrome (pSS) is a complex, multisystem autoimmune disorder. It is characterized by lymphocytic infiltration of the exocrine glands. In the setting of pSS, the presence of systemic disease is an important prognostic determinant, but involvement of the kidney is uncommon. The triad of pSS, distal renal tubular acidosis (dRTA), and central pontine myelinolysis (CPM) is rare and potentially fatal. A 42-year-old woman presented with dRTA, profound hypokalemia, and CPM characterized by progressive global quadriparesis, ophthalmoplegia, and encephalopathy. Sjögren's syndrome was diagnosed based on sicca symptoms, clinical features, and strongly positive anti-SSA/Ro and anti-SSB/La autoantibodies. The patient responded well to electrolyte replacement, acid-base correction, corticosteroids, and subsequent cyclophosphamide therapy. Early recognition and appropriate treatment resulted in good kidney and neurological outcomes in this case. This report highlights the need to consider the diagnosis of pSS in unexplained dRTA and CPM, as it has a favorable prognosis if recognized and managed timeously.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
