{"title":"乙型流感病毒感染后耐甲氧西林金黄色葡萄球菌并发急性心包炎和外周静脉导管相关血流感染1例报告。","authors":"Fumihiro Ochi, Hisamichi Tauchi, Hiromitsu Miura, Tomozo Moritani, Toshiyuki Chisaka, Takashi Higaki, Mariko Eguchi","doi":"10.1155/2023/4374552","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In this study, we report the case of a 14-month-old female patient transferred from another hospital to our hospital with a 9-day history of fever and worsening dyspnea. <i>Case Report</i>. The patient tested positive for influenza type B virus 7 days before being transferred to our hospital but was never treated. The physical examination performed at presentation revealed redness and swelling of the skin at the site of the peripheral venous catheter insertion performed at the previous hospital. Her electrocardiogram revealed ST segment elevations in leads II, III, aVF, and V2-V6. An emergent transthoracic echocardiogram revealed pericardial effusion. As ventricular dysfunction due to pericardial effusion was not present, pericardiocentesis was not performed. Furthermore, blood culture revealed methicillin-resistant <i>Staphylococcus aureus</i> (MRSA). Thus, a diagnosis of acute pericarditis complicated with sepsis and peripheral venous catheter-related bloodstream infection (PVC-BSI) due to MRSA was made. Frequent bedside ultrasound examinations were performed to evaluate the outcomes of the treatment. After administering vancomycin, aspirin, and colchicine, the patient's general condition stabilized.</p><p><strong>Conclusions: </strong>In children, it is crucial to identify the causative organism and provide appropriate targeted therapy to prevent worsening of the condition and mortality due to acute pericarditis. Moreover, it is important to carefully monitor the clinical course for the progression of acute pericarditis to cardiac tamponade and evaluate the treatment outcomes.</p>","PeriodicalId":9623,"journal":{"name":"Case Reports in Pediatrics","volume":"2023 ","pages":"4374552"},"PeriodicalIF":0.5000,"publicationDate":"2023-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10169241/pdf/","citationCount":"0","resultStr":"{\"title\":\"Complicated Acute Pericarditis and Peripheral Venous Catheter-Related Bloodstream Infection Caused by Methicillin-Resistant <i>Staphylococcus aureus</i> after Influenza B Virus Infection: A Case Report.\",\"authors\":\"Fumihiro Ochi, Hisamichi Tauchi, Hiromitsu Miura, Tomozo Moritani, Toshiyuki Chisaka, Takashi Higaki, Mariko Eguchi\",\"doi\":\"10.1155/2023/4374552\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In this study, we report the case of a 14-month-old female patient transferred from another hospital to our hospital with a 9-day history of fever and worsening dyspnea. <i>Case Report</i>. The patient tested positive for influenza type B virus 7 days before being transferred to our hospital but was never treated. The physical examination performed at presentation revealed redness and swelling of the skin at the site of the peripheral venous catheter insertion performed at the previous hospital. Her electrocardiogram revealed ST segment elevations in leads II, III, aVF, and V2-V6. An emergent transthoracic echocardiogram revealed pericardial effusion. As ventricular dysfunction due to pericardial effusion was not present, pericardiocentesis was not performed. Furthermore, blood culture revealed methicillin-resistant <i>Staphylococcus aureus</i> (MRSA). Thus, a diagnosis of acute pericarditis complicated with sepsis and peripheral venous catheter-related bloodstream infection (PVC-BSI) due to MRSA was made. Frequent bedside ultrasound examinations were performed to evaluate the outcomes of the treatment. After administering vancomycin, aspirin, and colchicine, the patient's general condition stabilized.</p><p><strong>Conclusions: </strong>In children, it is crucial to identify the causative organism and provide appropriate targeted therapy to prevent worsening of the condition and mortality due to acute pericarditis. Moreover, it is important to carefully monitor the clinical course for the progression of acute pericarditis to cardiac tamponade and evaluate the treatment outcomes.</p>\",\"PeriodicalId\":9623,\"journal\":{\"name\":\"Case Reports in Pediatrics\",\"volume\":\"2023 \",\"pages\":\"4374552\"},\"PeriodicalIF\":0.5000,\"publicationDate\":\"2023-05-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10169241/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Pediatrics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2023/4374552\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Pediatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2023/4374552","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"PEDIATRICS","Score":null,"Total":0}
Complicated Acute Pericarditis and Peripheral Venous Catheter-Related Bloodstream Infection Caused by Methicillin-Resistant Staphylococcus aureus after Influenza B Virus Infection: A Case Report.
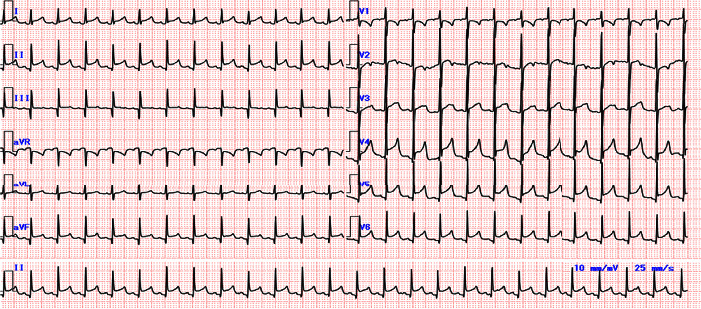
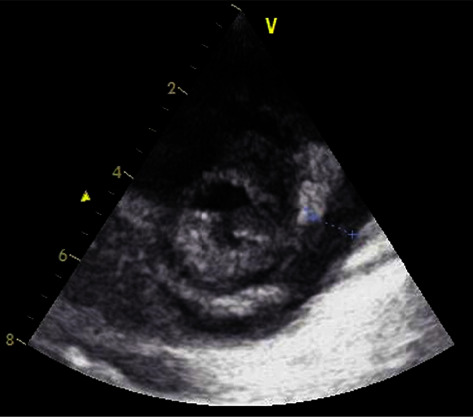
Background: In this study, we report the case of a 14-month-old female patient transferred from another hospital to our hospital with a 9-day history of fever and worsening dyspnea. Case Report. The patient tested positive for influenza type B virus 7 days before being transferred to our hospital but was never treated. The physical examination performed at presentation revealed redness and swelling of the skin at the site of the peripheral venous catheter insertion performed at the previous hospital. Her electrocardiogram revealed ST segment elevations in leads II, III, aVF, and V2-V6. An emergent transthoracic echocardiogram revealed pericardial effusion. As ventricular dysfunction due to pericardial effusion was not present, pericardiocentesis was not performed. Furthermore, blood culture revealed methicillin-resistant Staphylococcus aureus (MRSA). Thus, a diagnosis of acute pericarditis complicated with sepsis and peripheral venous catheter-related bloodstream infection (PVC-BSI) due to MRSA was made. Frequent bedside ultrasound examinations were performed to evaluate the outcomes of the treatment. After administering vancomycin, aspirin, and colchicine, the patient's general condition stabilized.
Conclusions: In children, it is crucial to identify the causative organism and provide appropriate targeted therapy to prevent worsening of the condition and mortality due to acute pericarditis. Moreover, it is important to carefully monitor the clinical course for the progression of acute pericarditis to cardiac tamponade and evaluate the treatment outcomes.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
